Your neck has been stiff for weeks. Some mornings, you wake up with a dull ache that spreads to your shoulders. You hear a grinding noise when you turn your head. You have searched online for “cervical pain symptoms” or “what is a cervical problem” – and landed here.
You are not alone.
Cervical spondylosis, commonly called arthritis of the neck, is one of the most widespread spinal conditions in the world. It affects more than 85% of people over the age of 60. In India, the numbers are growing faster than ever – especially among desk workers, IT professionals, and teachers – because of long hours spent hunched over screens and poor posture.
The good news: most people with cervical spondylosis do not need surgery. With the right diagnosis, treatment, and exercises, you can manage – and in many cases, significantly reduce – your cervical pain.
This guide will walk you through everything you need to know: what cervical spondylosis is, its symptoms, how it is diagnosed, the best medicines and exercises, and the honest answer to whether cervical spondylosis can be cured permanently.
Table of Contents
What is Cervical Spondylosis?
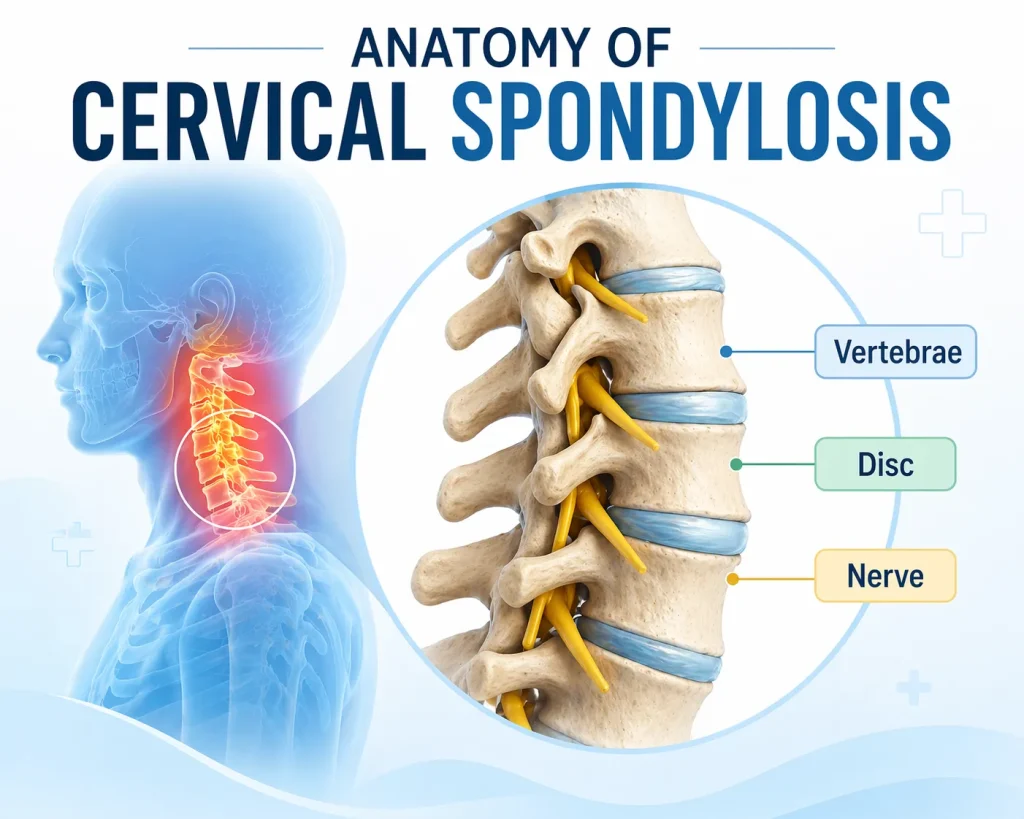
Cervical spondylosis is the medical term for age-related, wear-and-tear changes in the cervical spine – the seven vertebrae that form your neck.
Think of it this way: just like the soles of your shoes wear down over years of walking, the discs and joints in your neck wear down over years of movement, stress, and gravity. This is called degeneration – and it is a completely natural process.
The cervical spine consists of:
- Vertebrae – the bones that stack on top of each other to form the neck
- Intervertebral discs – soft, cushion-like pads between each vertebra that act as shock absorbers
- Spinal cord and nerve roots – the electrical cables that carry signals between your brain and body
- Facet joints – the small joints at the back of each vertebra that allow movement
When these structures degenerate, the discs lose height, dry out, and begin to bulge. The joints develop arthritis. Bone spurs – called osteophytes – may grow and press on nearby nerves or the spinal cord. This is the root of cervical spondylosis.
Cervical Spondylosis vs Spondylitis – What Is the Difference?
These two terms are often confused:
- Cervical spondylosis refers to degenerative changes caused by ageing and wear
- Cervical spondylitis refers to inflammation in the cervical spine, often linked to conditions like ankylosing spondylitis, an autoimmune disease
In everyday conversation, many people in India use “cervical” as shorthand for any neck pain. Medically, cervical spondylosis and spondylitis are distinct – though their symptoms can overlap.
Who Gets Cervical Spondylosis? Risk Factors Explained
Cervical spondylosis is extremely common. Radiographic studies – meaning X-rays and MRI scans – show degenerative changes in approximately 25% of people under 40, 50% of those over 40, and up to 85–95% of individuals over 65.
However, not everyone with these changes experiences symptoms.
Common risk factors include:
- Age – the most significant factor. Most people experience symptoms after their fifth decade of life
- Occupation – teachers, IT professionals, surgeons, and computer users are at high risk. One Indian study found that 88.32% of computer users reported neck-related musculoskeletal complaints
- Genetics – a family history of neck pain and spondylosis increases your risk
- Smoking – clearly linked to increased neck pain and faster disc degeneration
- Previous neck injury or trauma – old injuries can accelerate degenerative changes
- Sedentary lifestyle and obesity – excess body mass increases compressive forces on cervical discs
- Poor posture – prolonged neck flexion (looking down at a phone) and forward head posture accelerate early degenerative changes in the cervical spine
- Anxiety and depression – mental health conditions are associated with heightened perception of cervical pain
Early cervical spondylosis can appear as early as your 30s, especially in high-risk occupations. Early spondylotic changes on an X-ray mean that disc degeneration has begun – this does not always mean you will develop symptoms.
Cervical Spondylosis Symptoms: What to Look For

For many people, cervical spondylosis causes no noticeable symptoms at all. When symptoms do appear, they can vary widely in severity.
The most common cervical spondylosis symptoms include:
- Neck pain and stiffness – can range from mild to severe; often worse after sitting or sleeping in one position
- Cervical spondylosis pain areas – pain is typically felt in the neck, but can radiate to the shoulders, upper back, and arms
- Grinding or popping sensation – a grating noise or feeling when turning the neck (crepitus)
- Headaches – cervical spondylosis headaches usually begin at the base of the skull and radiate toward the forehead. Yes, cervical spondylosis can cause headaches – this is called cervicogenic headache
- Numbness or tingling – in the arms, hands, and fingers, when nerve roots are compressed (cervical radiculopathy)
- Weakness in the hands or arms – difficulty with fine motor tasks like writing or buttoning a shirt
- Muscle spasms in the neck and shoulders
More serious symptoms that need urgent attention:

- Trouble walking or loss of balance
- Weakness in the legs
- Loss of bladder or bowel control
These may indicate cervical spondylotic myelopathy – compression of the spinal cord itself – which requires immediate medical evaluation.
Can Cervical Spondylosis Cause Headaches?

Yes – and this is one of the most commonly asked questions. Cervical spondylosis headache occurs because degenerated discs and inflamed joints irritate the upper cervical nerve roots, which refer pain to the head. The C2 and C3 nerve roots in particular share pathways with pain-sensitive structures in the skull. If you experience recurring headaches alongside neck stiffness, ask your spine specialist about cervicogenic headache as part of your cervical spondylosis diagnosis.
Can Cervical Spondylosis Cause High Blood Pressure?
Some research suggests a possible relationship between upper cervical spine dysfunction and blood pressure regulation. However, this is not a confirmed direct cause. If you have hypertension alongside cervical symptoms, discuss both with your physician.
Cervical Spondylitis Symptoms in Females
Women often report cervical spondylosis symptoms slightly differently – with more emphasis on headaches, dizziness, nausea, and shoulder blade pain alongside classic neck stiffness. Hormonal factors and differences in spinal anatomy may contribute to how symptoms present in women.
Cervical Spondylosis Diagnosis: Tests and Imaging
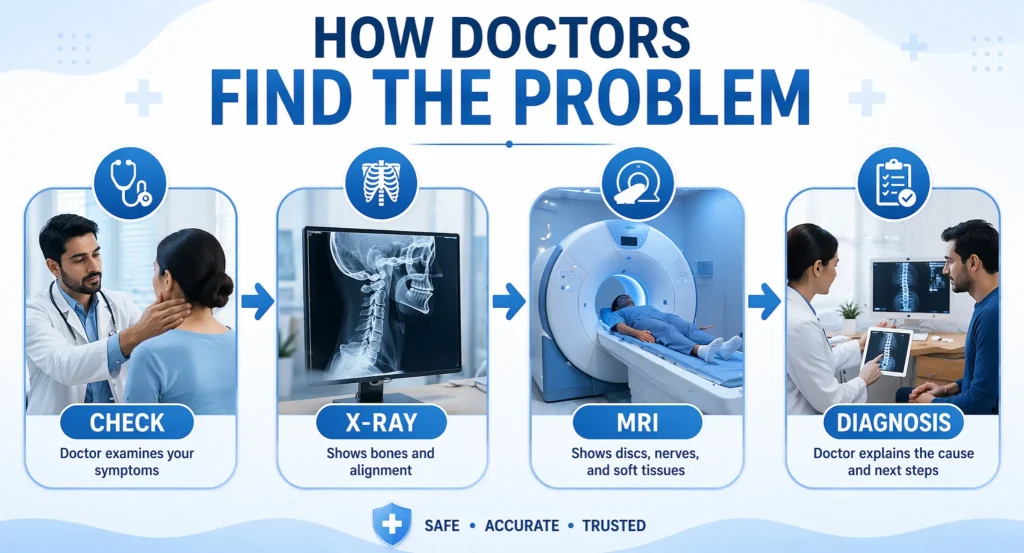
How Is Cervical Spondylosis Diagnosed?
Your doctor will begin with a thorough physical examination of your neck, shoulders, and arms, testing for:
- Strength in the arms, hands, and fingers
- Touch sensation and reflexes
- Range of motion and flexibility
- Gait (how you walk)
They will also ask for a detailed history: when the pain started, what makes it worse, whether you have numbness or weakness, and any previous neck injuries.
Diagnostic Tests for Cervical Spondylosis:
- X-ray (cervical spondylosis X-ray) – the first-line imaging test. A cervical spondylitis X-ray shows bone alignment, loss of disc height, bone spurs, and early spondylotic changes. It is simple, affordable, and widely available across India
- MRI (Magnetic Resonance Imaging) – the gold standard for soft tissue assessment. Cervical spondylosis MRI shows disc herniation, nerve root compression, and spinal cord involvement in detail
- CT scan – provides a more detailed view of bone structures and the spinal canal than X-ray alone
- Myelogram – contrast dye is injected into the spinal canal for detailed nerve imaging, usually combined with CT
- Electrodiagnostic testing (EMG/NCS) – measures electrical impulses in muscles and nerves to determine if a specific nerve root is compressed
- Blood tests – to rule out rheumatoid arthritis or other inflammatory arthritis conditions
Cervical Spondylosis Differential Diagnosis
Several conditions can mimic cervical spondylosis symptoms, including:
- Rheumatoid arthritis of the cervical spine (cervical ankylosing spondylitis)
- Cervical disc herniation without spondylosis
- Fibromyalgia
- Thoracic outlet syndrome
- Shoulder pathology (rotator cuff problems)
This is why a precise diagnosis from a qualified spine specialist matters before starting any treatment.
Cervical Spondylosis Treatment: A Complete Guide

The majority of cervical spondylosis cases – including mild cervical spondylosis and moderate cases – respond well to non-surgical treatment. Surgery is reserved for specific, serious situations.
Non-Surgical (Conservative) Treatment
1. Physical Therapy
Physical therapy is typically the first treatment your doctor will recommend. A structured programme – usually 6 to 8 weeks, with 2 to 3 sessions per week – focuses on:
- Strengthening the deep neck flexor muscles
- Improving posture and ergonomics
- Stretching tight muscles in the neck and shoulders
- Cervical traction – gently stretching the joints and muscles of the neck to relieve nerve compression
- Postural correction for those with loss of cervical lordosis (flattening of the natural neck curve)
Cervical Spondylosis Exercises With Pictures (Summary)

These are the core exercises recommended. Always perform these gently and stop if pain worsens:
- Chin tucks – pull your chin straight back, making a “double chin.” Hold 5 seconds. Repeat 10 times. This restores cervical lordosis and relieves forward head posture
- Neck rotations – slowly turn your head to the left, hold 5 seconds, return to centre, then right. Repeat 5 times each side
- Shoulder blade squeezes – sit straight, squeeze shoulder blades together and hold 5 seconds. Repeat 10 times
- Cervical side bends – gently tilt your head toward your shoulder without lifting the shoulder. Hold 5 seconds. Alternate sides
- Levator scapulae stretch – tilt your head forward and to one side, apply gentle pressure with your hand, hold 20 seconds on each side
Note: These cervical stretches are general guidelines. A physiotherapist will tailor exercises to your specific level of degeneration and symptoms. Do not begin an exercise programme without professional guidance if you have severe symptoms or suspected myelopathy.
2. Medications
Your doctor may prescribe a combination of medicines during the acute phase:
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) – such as ibuprofen and naproxen. These are considered first-line medications for cervical pain, addressing both pain and inflammation. These are among the most commonly recommended cervical pain medicine options in India
- Acetaminophen (Paracetamol) – for mild pain relief
- Oral corticosteroids – a short course to rapidly reduce inflammation during a flare
- Muscle relaxants – such as cyclobenzaprine, to relieve painful muscle spasms in the neck and shoulders
- Neuropathic pain agents – such as pregabalin or gabapentin, used when there is nerve root involvement with tingling and numbness
- Topical agents – neck pain relief patches and topical anti-inflammatory gels can provide localised relief
Best Medicine for Cervical Spondylosis
There is no single “best” medicine for cervical spondylosis – the ideal choice depends on whether your dominant symptoms are pain, inflammation, muscle spasm, or nerve compression. Your spine specialist will prescribe the most appropriate cervical spondylosis medicine name based on your condition. Self-medicating without a diagnosis is not advisable and can mask serious nerve compression.
A note on homoeopathic medicine for cervical pain: While some patients report relief with homoeopathic remedies, there is currently insufficient clinical evidence to support their use as a primary treatment for cervical spondylosis. Always discuss any supplements or alternative treatments with your treating physician.
3. Cervical Collar (Neck Support)
A soft cervical collar – a padded ring that wraps around the neck – can be prescribed for short-term use to limit neck motion and allow muscles to rest. The best neck support for cervical spondylosis is one fitted by a physiotherapist. Long-term use is discouraged, as it weakens neck muscles over time.
4. Steroid Injections
When medications and therapy fail to provide adequate relief, targeted injections offer more direct pain management:
- Cervical epidural block – steroid and anaesthetic injected into the epidural space, effective for radiculopathy (pinched nerve causing arm pain)
- Cervical facet joint block – injection into the facet joint capsule for arthritis-driven neck pain
- Radiofrequency ablation – in chronic cervical pain, the nerve supplying the painful facet joint is blocked and then ablated (burned) to provide pain relief lasting several months
5. Lifestyle Modifications
- Best pillow for neck arthritis: Use a cervical contour pillow that maintains natural neck curvature during sleep. For those with loss of cervical lordosis, a pillow that gently supports the neck’s natural curve is ideal
- How to sleep with loss of cervical lordosis: Sleep on your back with a cervical roll pillow under your neck, or on your side with a pillow that keeps your spine aligned. Avoid sleeping on your stomach
- Cervical spondylosis foods to avoid: While no specific diet cures spondylosis, anti-inflammatory eating helps. Reduce processed foods, refined sugars, and trans fats. Increase omega-3 fatty acids (fish, flaxseed), turmeric, and leafy greens
- Oil for cervical pain: Warm sesame oil, eucalyptus oil, and wintergreen oil can provide temporary topical relief through improved local circulation
- Ergonomics: Keep your computer screen at eye level. Take breaks every 30-45 minutes. Avoid prolonged neck flexion (looking down at your phone for extended periods – sometimes called “text neck”)
Surgical Treatment for Cervical Spondylosis
Surgery is not commonly recommended for cervical spondylosis. It is considered when:
- A spinal nerve is being pinched by a herniated disc or bone spur (cervical radiculopathy), and conservative treatment has failed
- The spinal cord is being compressed (cervical spondylotic myelopathy)
- There is progressive neurological deterioration – worsening arm weakness, unsteadiness, or falling
Surgical options include:
- Anterior Cervical Discectomy and Fusion (ACDF) – the most common surgical procedure; the damaged disc is removed and the vertebrae above and below are fused
- Cervical disc arthroplasty – replacement of the damaged disc with an artificial disc, preserving motion
- Posterior laminoplasty – the back of the spinal canal is widened to relieve pressure on the spinal cord
The decision between surgical and non-surgical treatment should be made by an experienced spine surgeon after thorough evaluation. Not all patients with severe neck pain are surgical candidates – widespread arthritis, other medical conditions, or non-spinal causes of pain may make surgery inappropriate.
Can Cervical Spondylosis Be Cured Permanently?
This is the question most patients ask first.
The honest answer: cervical spondylosis itself – the degenerative changes in the disc and joints – cannot be fully reversed. It is a natural ageing process. The structural changes on an X-ray or MRI will not disappear.
However – and this is important – most people with cervical spondylosis achieve excellent long-term symptom control and live completely normal lives.
With the right treatment:
- Pain can be significantly reduced or eliminated
- Nerve symptoms (numbness, tingling) can resolve
- Function and quality of life can be fully restored
- Disease progression can be slowed with exercise, posture correction, and lifestyle changes
The goal of treatment is not to reverse the clock on your spine – it is to give you your life back. Many patients with mild cervical spondylosis or even moderate cervical spondylosis with degenerative disc disease achieve complete symptom resolution through physical therapy and medications alone.
Early cervical spondylosis – when caught and treated before significant nerve involvement – has the best long-term prognosis. This underlines the importance of not ignoring persistent cervical pain symptoms.
Early Degenerative Changes in the Cervical Spine: Should You Be Worried?
If your X-ray or MRI report says “early spondylotic changes” or “early degenerative changes in cervical spine” – do not panic.
This finding simply means the normal aging process has begun in your cervical discs and joints. It does not mean your condition will worsen dramatically, and it does not mean you need surgery.
What does it mean:
- This is a good time to start a posture correction and strengthening programme
- Adopt ergonomic habits now – they will significantly slow progression
- Discuss your results with a spine specialist rather than self-diagnosing
Cervical Spondylosis C5-C6: A Common Level Explained
The C5-C6 level is the most commonly affected segment in cervical spondylosis, followed by C6-C7.
Why C5-C6? This segment bears the greatest mechanical load and has the highest range of motion in the mid-cervical spine, making it most vulnerable to degenerative wear.
Cervical spondylosis C5-C6 symptoms include:
- Neck pain radiating to the shoulder and outer arm
- Numbness or tingling in the thumb and index finger (C6 dermatome)
- Weakness in the bicep muscle
- Reduced bicep reflex
C6-C7 symptoms include:
- Pain radiating into the middle and ring fingers
- Tricep weakness
- Reduced tricep reflex
Identifying the affected level of imaging helps guide targeted treatment – whether physiotherapy, injections, or surgery at that specific spinal segment.
Conclusion: Taking Control of Your Cervical Health
Cervical spondylosis – arthritis of the neck – is not a life sentence. It is one of the most common and most manageable conditions in spine medicine.
Key takeaways from this guide:
- Cervical spondylosis is age-related wear and tear in the seven vertebrae of the neck
- It affects the majority of people over 60, though symptoms are not always present
- Common symptoms include neck pain, stiffness, cervical headaches, numbness in the arms, and muscle spasms
- Diagnosis is confirmed through physical examination, X-ray, and MRI
- Most cases respond well to physical therapy, medications, posture correction, and lifestyle changes
- Surgery is reserved for spinal cord compression or progressive nerve damage
- While the degenerative changes cannot be fully reversed, symptoms can be effectively controlled
- Early detection and early treatment deliver the best long-term outcomes
If you have been experiencing persistent neck pain, stiffness, or radiating arm symptoms, do not wait. A precise diagnosis from a qualified spine specialist is the most important first step toward relief.
FAQs
What is cervical spondylosis?
Cervical spondylosis is an age-related degeneration of the discs and joints in the cervical spine (neck), causing neck pain, stiffness, and sometimes nerve compression. It affects more than 85% of people over age 60.
What are the main cervical spondylosis symptoms?
The most common symptoms are neck pain and stiffness, grinding sensations, shoulder pain, headaches, and numbness or tingling in the arms and fingers. Severe cases may cause difficulty walking.
Can cervical spondylosis be cured permanently?
The structural degeneration cannot be fully reversed. However, symptoms can be effectively managed with therapy, medication, and lifestyle changes, allowing most patients to live pain-free, normal lives.
What is the difference between cervical spondylosis and spondylitis?
Spondylosis refers to degenerative wear-and-tear changes. Spondylitis refers to inflammatory conditions, often autoimmune in origin. They can share symptoms but have different causes and treatments.
Does cervical spondylosis cause headaches?
Yes. Cervical spondylosis can cause headaches – called cervicogenic headaches – that start at the base of the skull and radiate to the forehead, due to irritation of the upper cervical nerve roots.
What is the best medicine for cervical spondylosis?
NSAIDs like ibuprofen and naproxen are first-line cervical pain medicines. Muscle relaxants, neuropathic agents, and short-course steroids may be added based on your specific symptoms. Always consult a spine specialist.
How is cervical spondylosis diagnosed?
Through clinical examination, X-ray (to detect bone spurs and disc height loss), and MRI (to assess soft tissue, discs, and nerve involvement). Blood tests may rule out inflammatory arthritis.
What exercises help cervical spondylosis?
Chin tucks, gentle neck rotations, shoulder blade squeezes, cervical side bends, and levator scapulae stretches are recommended. Always begin under physiotherapist’s supervision to avoid worsening symptoms.
What is C5-C6 cervical spondylosis?
C5-C6 is the most commonly affected spinal level in cervical spondylosis. It can cause radiating pain into the shoulder and outer arm, thumb and index finger numbness, and bicep weakness.
When does cervical spondylosis require surgery?
Surgery is considered when the spinal cord is compressed (myelopathy), when a pinched nerve causes progressive weakness, or when conservative treatment has failed after several months. Most cases do not need surgery.