Key Takeaways:
- Knee arthritis happens when the protective cartilage inside your knee slowly wears away, causing pain, swelling, and stiffness over time.
- There are three main types: Osteoarthritis from wear and tear, Rheumatoid Arthritis from an immune system attack, and Posttraumatic Arthritis from old injuries.
- Early warning signs include morning stiffness, a creaking sensation in the knee, swelling, and pain that gets worse after being active.
- Treatment starts without surgery, using physiotherapy, weight loss, and medications. Surgery, like knee replacement, is only considered for very advanced cases.
- Keeping a healthy body weight is the single most effective way to protect your knees, since extra weight puts much more pressure on the joint.
Your knees carry your body weight every single day. Walking to the market, climbing stairs, sitting cross-legged – the knee joint is always at work.
So when that familiar ache begins – especially in the morning, after a long car ride, or while climbing stairs – it is natural to wonder: Is this just age? Or is it something more serious?
Knee arthritis is one of the most common joint conditions in India, affecting millions of people above the age of 40. Yet many patients delay seeking help because they do not fully understand what is happening inside their knee joint.
This guide covers everything you need to know – what knee arthritis is, why it happens, how to recognise the early symptoms, and what modern treatment options can offer. Whether you have been recently diagnosed or are still figuring out what is causing your pain, this is your starting point.
Table of Contents
What is Arthritis of the Knee?
Arthritis simply means inflammation of a joint. When it affects the knee, the result is pain, swelling, stiffness, and a gradual loss of smooth movement that makes everyday life harder.
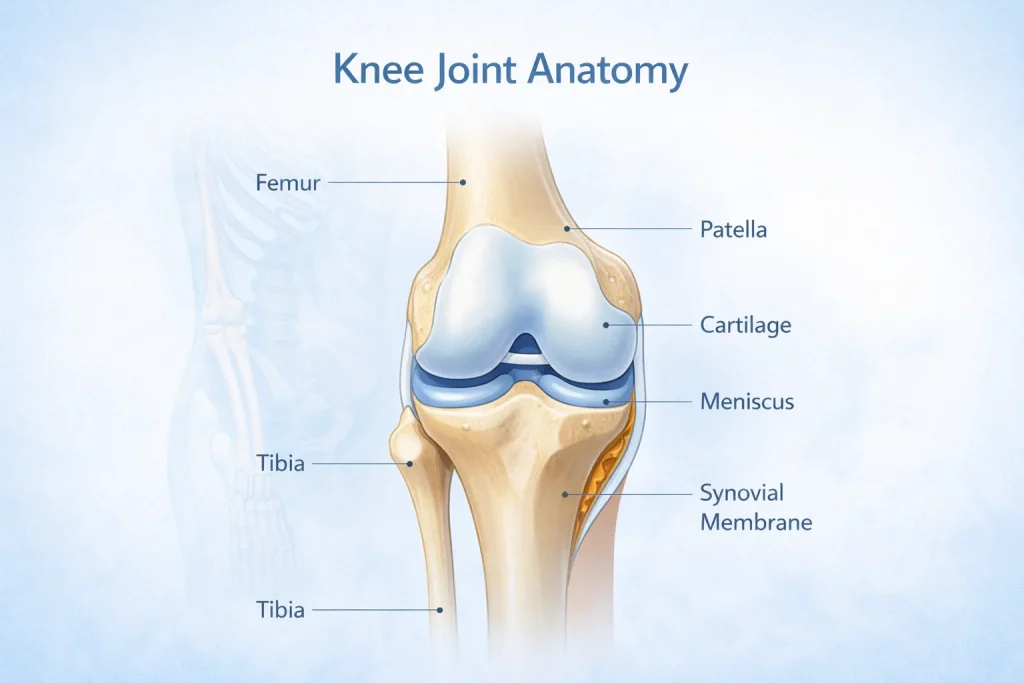
The knee is the largest and strongest joint in the human body. It is formed by three bones:
- The femur (thighbone) – the upper part
- The tibia (shinbone) – the lower part
- The patella (kneecap) – sits at the front of the joint
These bones are covered by articular cartilage – a smooth, slippery material that allows the knee to bend and straighten without friction. Two wedge-shaped pads called the meniscus act as shock absorbers between the thighbone and shinbone. A thin lining called the synovial membrane releases lubricating fluid to keep the joint moving smoothly.
When arthritis develops, this carefully balanced system breaks down. The cartilage wears away, the space between bones narrows, inflammation sets in, and normal movement becomes painful.
There is no permanent cure for knee arthritis. But with the right care, most patients manage their pain well and continue living an active life.
How the Knee Joint Works
Think of the knee as a well-oiled hinge. For it to work properly, every component – cartilage, meniscus, ligaments, tendons, and synovial fluid – must function together. When even one part degenerates, the entire system suffers. This is why knee joint diseases such as arthritis have such a significant impact on daily life.
Types of Knee Arthritis
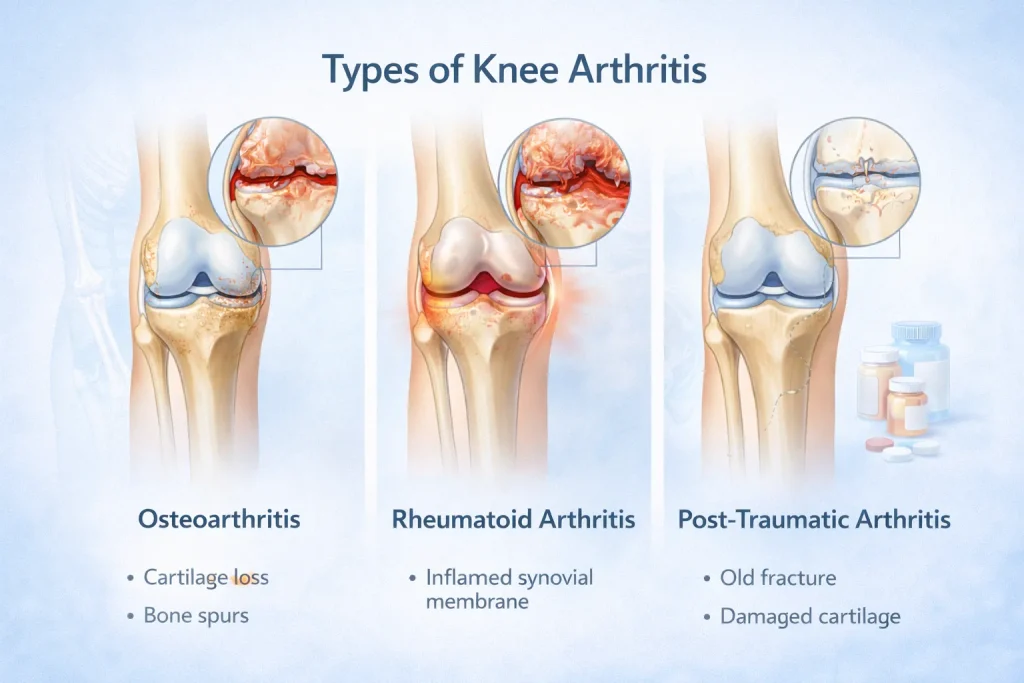
There are more than 100 types of arthritis, but three main types affect the knee joint. Understanding which type you have is the first step toward the right treatment.
1. Osteoarthritis (OA Knee) – The Most Common Type
Osteoarthritis is by far the most common form of knee arthritis, especially in adults above 50. It is often called degenerative arthritis or wear-and-tear arthritis because the cartilage inside the knee gradually breaks down over time.
In OA knee, the cartilage becomes frayed and rough. As it wears further, the protective space between the bones decreases. In severe cases, the bones begin rubbing directly against each other. This is what causes the deep, aching knee joint pain that worsens over the years.
Bone spurs – also called osteophytes – often form around the joint as the body tries to compensate for cartilage loss. These are clearly visible on an OA knee X-ray and are one of the defining signs of advanced osteoarthritis of the knee.
Key facts about OA Knee:
- OA knee full form: Osteoarthritis of the Knee
- Can affect one knee (left knee OA or right knee OA) or both (bilateral knee osteoarthritis)
- Develops slowly – from mild OA knee to severe OA knee over months and years
- Most common in middle-aged and older adults, especially women after menopause
- Classified into stages based on how much cartilage and joint space have been lost
2. Rheumatoid Arthritis (RA) in the Knee
Rheumatoid arthritis is an autoimmune disease. The body’s immune system mistakenly attacks the synovial membrane lining the knee joint. This causes persistent inflammation, rheumatoid arthritis, knee pain, and progressive joint damage.
Unlike osteoarthritis, RA in the knees is symmetrical – it typically affects both knees at the same time. RA can develop at any age, including in young adults.
In RA knee, the inflamed synovial membrane gradually damages the cartilage and softens the underlying bone. Without proper treatment, rheumatoid arthritis can cause serious joint damage and visible knee deformity.
Key differences between RA and OA in the knees:
- RA is driven by the immune system; OA is driven by mechanical wear
- Rheumatoid arthritis knee symptoms include stiffness that is worst in the morning and improves with movement
- RA often affects multiple joints at the same time; OA may be limited to the knee
- Blood tests are essential to confirm RA; X-rays alone are not sufficient
3. Posttraumatic Arthritis
This type develops after a direct injury to the knee, such as a fracture, torn meniscus, or ligament damage. Even when the original injury heals, the joint surface may be damaged in a way that leads to arthritis years or even decades later.
Athletes, manual labourers, and people with a history of significant knee injuries carry a much higher risk. The wear-and-tear process accelerates after trauma, causing degenerative changes in the knee far earlier than normal ageing would cause.
What Causes Knee Arthritis?

Why does arthritis occur in the knee? The answer depends on the type. Here are the main causes and risk factors behind knee joint degeneration:
- Age: The most significant risk factor. Cartilage naturally degrades over time. OA knee is most common after the age of 50.
- Excess body weight: Every extra kilogram adds approximately 4 to 5 kg of additional load on the knee joint. Weight loss is one of the most effective ways to slow OA knee progression.
- Previous knee injury: Meniscal tears, ligament injuries, and fractures increase the long-term risk of posttraumatic arthritis significantly.
- Genetics: A family history of arthritis raises your risk, particularly for OA and RA.
- Gender: Women are at higher risk of developing knee OA, especially after menopause.
- Occupation: Jobs involving prolonged kneeling, squatting, or heavy lifting accelerate knee joint degeneration over the years.
- Autoimmune factors: For rheumatoid arthritis, genetic and environmental triggers cause the immune system to attack joint tissues.
Early Symptoms of Arthritis in the Knee

Recognising the early symptoms of arthritis in the knees gives you the best chance to act before significant joint damage occurs. Many patients dismiss these signs as normal ageing – which delays diagnosis and treatment.
Common OA knee symptoms and RA knee symptoms include:
- Morning stiffness: A stiff knee joint after sleep or after sitting for a long period is often the earliest warning sign. It typically eases within 30 minutes of moving around.
- Pain during or after activity: Knee arthritis pain initially flares during vigorous movement and settles with rest. In later stages, pain may be present even at rest.
- Knee joint pain and swelling: Arthritis knee swelling occurs as the joint produces excess fluid in response to inflammation. The knee may feel warm, tight, and puffy.
- Creaking or grinding: A grating sound or sensation called crepitus when bending the knee is a sign of cartilage damage. The knee may also click, snap, or lock during movement.
- Reduced range of motion: Bending or fully straightening the knee becomes difficult. Climbing stairs and rising from a low chair grow progressively harder.
- Weakness or buckling: The knee may feel unstable, as though it might give way under body weight.
- Pain with weather changes: Many arthritis patients notice that knee joint pain worsens in cold or rainy weather – a well-recognised pattern in OA knee.
In rheumatoid arthritis, additional symptoms may include fatigue, a mild fever, and pain or swelling in other joints such as the wrists and fingers.
Stages of Knee Osteoarthritis
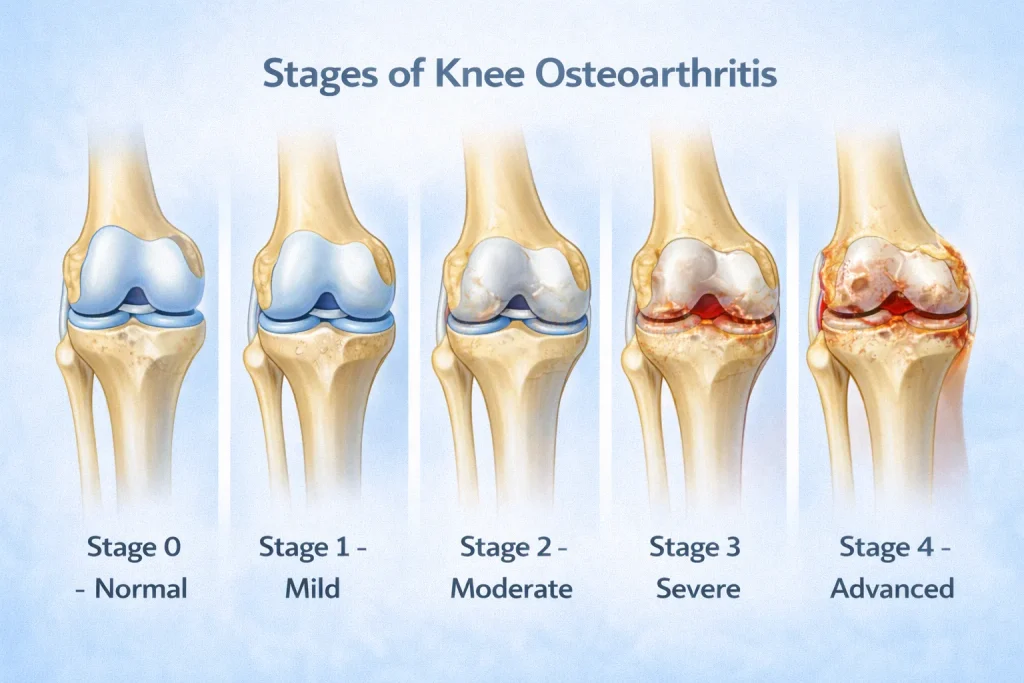
OA knee progresses through clearly defined stages. Understanding the stages of knee osteoarthritis helps both doctors and patients decide on the right treatment at the right time.
Stage 0 – Normal, No arthritis. Normal knee joint space. No cartilage damage visible on X-ray.
Stage 1 – Mild OA Knee, Minor bone spur growth begins. Cartilage is still largely intact. Minimal or no pain at this stage.
Stage 2 – Moderate Osteoarthritis, More osteophytes are visible. Cartilage thinning begins. Pain becomes noticeable, especially after activity.
Stage 3 – Severe OA Knee, Significant cartilage loss. Knee gap symptoms are visible on X-ray. Frequent pain during activity and sometimes at rest.
Stage 4 – Advanced Osteoarthritis, Knee joint space is severely reduced or completely absent. Bone-on-bone contact occurs. Severe knee joint pain with very limited function.
Tricompartmental osteoarthritis means arthritis has damaged all three compartments of the knee – the medial, lateral, and patellofemoral areas. This is advanced OA and almost always requires surgical evaluation.
When both knees reach this level of damage, it is referred to as advanced bilateral knee osteoarthritis – a condition that is very common among older patients in India.
How is Knee Arthritis Diagnosed?
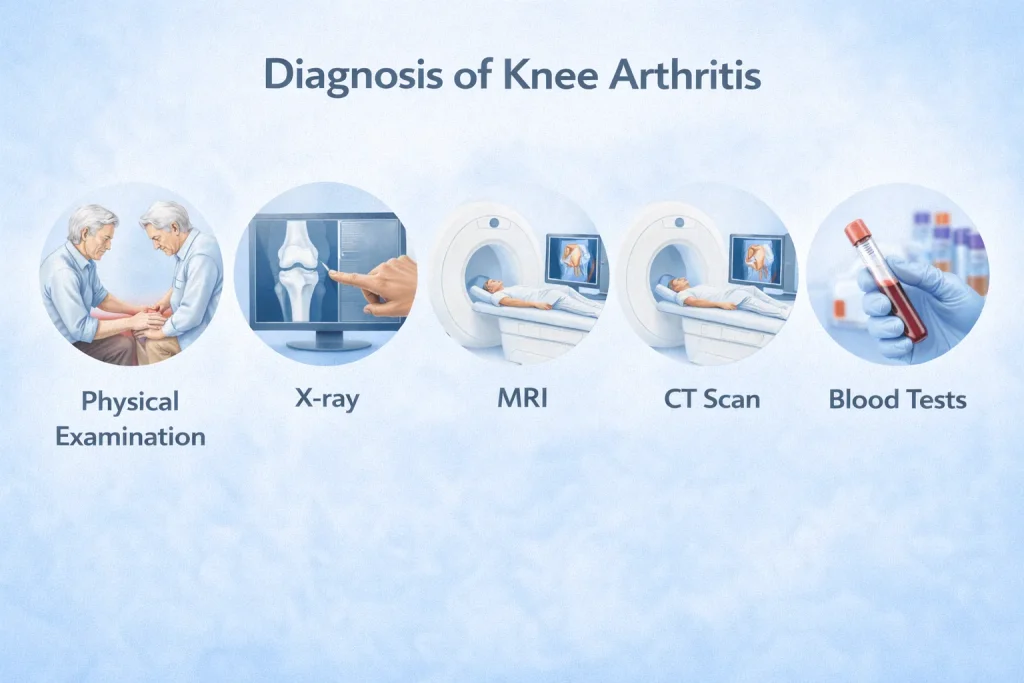
Diagnosis is not based on pain alone. Your orthopaedic specialist will use a combination of clinical history, physical examination, imaging investigations, and laboratory tests to confirm the diagnosis and understand its severity.
Physical Examination
During the consultation, your doctor will check:
- Swelling, warmth, or redness around the knee
- Tenderness when pressing around the joint line
- Range of motion – how far you can bend and straighten the knee
- Crepitus – the grating or grinding sensation inside the joint
- Instability – whether the knee wobbles or gives way under pressure
- Your gait – how you walk and whether you favour one side
- Whether other joints are involved, which may suggest rheumatoid arthritis
Imaging Tests: X-Ray, MRI, CT Scan
X-ray (OA knee X-ray / arthritic knee X-ray): The standard investigation for knee arthritis. An arthritic knee X-ray shows narrowing of the knee joint space, changes in the bone structure, and the presence of osteophytes. A normal knee joint space appears as a clearly visible gap between bones. When this gap is reduced or absent, it confirms cartilage loss and arthritis.
MRI (osteoarthritis knee MRI): Provides detailed imaging of soft tissues, including cartilage, meniscus, and ligaments. Particularly useful for detecting early OA changes that an X-ray may miss.
CT Scan: Used in complex cases to assess bone anatomy in greater detail, especially before surgical planning.
Laboratory Tests
Blood tests are especially important when rheumatoid arthritis is suspected. Markers such as Rheumatoid Factor (RF), Anti-CCP antibody, CRP, and ESR help confirm the RA diagnosis and guide the choice of medications. For OA knee, blood tests are usually normal, which itself helps rule out other types of arthritis.
Treatment Options for Knee Arthritis

There is no permanent cure for arthritis. But effective treatment can significantly reduce pain, improve function, and help you maintain an active life. Treatment is always personalised based on the type of arthritis, its stage, your age, and your overall health.
Non-Surgical Treatments
The vast majority of patients with knee arthritis – especially in early and moderate stages – are successfully managed without surgery. Non-surgical care is the foundation of knee arthritis treatment.
Lifestyle Modifications
These are among the most powerful tools available:
- Weight management: Losing even a few kilograms significantly reduces the load on the knee joint and slows OA progression.
- Activity modification: Switch from high-impact activities like running and jumping to low-impact alternatives such as swimming, cycling, and walking.
- Avoid activities that aggravate the joint – prolonged stair climbing, deep squatting, and kneeling.
- Balance, agility, and coordination exercises improve knee function and walking speed over time.
Physical Therapy
Osteoarthritis physiotherapy exercises are specifically designed to:
- Strengthen the muscles around the knee – especially the quadriceps and hamstrings
- Improve joint flexibility and range of motion
- Reduce mechanical stress on the knee during daily activities
A physiotherapist will design an individualised programme based on your stage of arthritis. Consistent physiotherapy can delay or even prevent the need for surgery in many patients.
Assistive Devices
Knee braces – both unloader and support types – along with walking canes and supportive footwear help stabilise the joint, reduce pain during movement, and improve confidence while walking.
Hot and Cold Therapy
Applying ice packs reduces acute swelling. Heat pads relax stiff muscles around the joint. Both provide practical, short-term relief from arthritis pain and inflammation.
Medications for Knee Arthritis
Your doctor will carefully select medications based on your specific health profile and the type of arthritis you have.
- NSAIDs (Non-Steroidal Anti-Inflammatory Drugs): Such as ibuprofen and naproxen. Available as oral tablets and topical gels. Effective for reducing knee inflammation and arthritis pain. Always use under medical guidance – particularly in patients with heart, kidney, or stomach conditions.
- Acetaminophen (Paracetamol): A safe and effective pain reliever for patients who cannot tolerate NSAIDs.
- COX-2 Inhibitors: A specialised class of NSAID – such as celecoxib and meloxicam, that provides anti-inflammatory benefits with fewer gastrointestinal side effects.
- Corticosteroid Injections: Powerful anti-inflammatory injections delivered directly into the knee joint. They provide significant but temporary pain relief. Because repeated injections can cause long-term joint damage, your doctor will limit their use.
- DMARDs (for Rheumatoid Arthritis): Disease-modifying drugs such as methotrexate, sulfasalazine, and hydroxychloroquine slow the progression of RA. Biologic agents such as etanercept and adalimumab reduce the immune system’s overactive response. These medications require specialist rheumatology management.
- Viscosupplementation: Hyaluronic acid injections into the knee supplement the joint’s natural lubricating fluid. They may improve pain and mobility in certain OA patients.
Important note on opioids: Oral narcotic medications are not recommended for knee arthritis pain. They are ineffective for this type of pain and carry serious risks.
On glucosamine and chondroitin: These supplements are widely used in India, but current clinical evidence does not confirm that they slow or reverse OA progression. Always discuss with your doctor before starting any supplement.
Surgical Treatment Options
Surgery is considered when arthritis is advanced, pain is severely disabling, and conservative treatments have not provided enough relief.
- Arthroscopy: Minimally invasive keyhole surgery. Used primarily when a degenerative meniscal tear accompanies OA of the knee. Not the main treatment for arthritis itself.
- Osteotomy: The shinbone or thighbone is cut and reshaped to shift body weight away from the damaged part of the knee. Best suited for younger, active patients with early-stage OA limited to one side of the joint.
- Cartilage Grafting: Healthy cartilage fills damaged areas in the joint. Suitable for younger patients with small, localised cartilage defects.
- Synovectomy: The inflamed joint lining is surgically removed. Used primarily in rheumatoid arthritis to reduce inflammation and slow joint damage.
- Partial Knee Replacement (Unicompartmental Arthroplasty): Only the damaged compartment of the knee is replaced. Requires a smaller incision and allows faster recovery.
- Total Knee Replacement (TKR): The definitive surgical option for severe OA knee and advanced bilateral knee osteoarthritis. Damaged bone and cartilage are removed and replaced with precision-fitted metal and plastic components. Most patients achieve significant pain relief and return to daily activities within weeks.
Expert Insight from deformity.co.in: Surgery is not a failure – it is a carefully timed tool. The goal is always to start with the least invasive approach and escalate only when necessary. Many patients with bilateral knee OA live comfortably for years on physiotherapy, weight management, and medication before surgery is ever considered. When surgery becomes necessary, timing matters – operating before deformity becomes severe leads to better outcomes and faster recovery.
Bilateral Knee Osteoarthritis: When Both Knees Are Affected
Bilateral knee osteoarthritis – OA in both knees simultaneously – is particularly common in India. Lifestyle factors, including floor-sitting, squatting, using Indian-style toilets, and physically demanding work, place intense and repeated stress on the knee joints over many years.
When both knees are affected:
- Patients often compensate by shifting their weight, which can worsen deformity over time
- The gait changes – a characteristic bent-knee or waddling walk develops gradually
- Daily tasks become progressively harder: walking, rising from a chair, using the toilet independently
- Both knees may need to be treated simultaneously or in a planned staged approach
The encouraging reality is that bilateral knee OA is very treatable. With the right combination of physiotherapy, weight management, medication, injections, and – when needed – bilateral knee replacement, patients can dramatically regain their quality of life and independence.
Knee Arthritis vs. Osteoporosis of the Knee

These two conditions are frequently confused, but they are distinct diseases with different causes and treatments – though they can coexist in the same person.
Knee Arthritis (Osteoarthritis): Involves the degeneration of the cartilage that covers the ends of the bones inside the knee joint. The primary problem is the joint surface breaking down. On an OA knee X-ray, reduced joint space and bone spurs are visible.
Osteoporosis Knee: Involves a loss of bone density throughout the body, including the bones that form the knee. The bones become weaker and more prone to fractures. Osteoporosis itself does not directly cause knee joint pain – but it dramatically increases the risk of fractures even from minor falls.
Key differences:
- Arthritis damages the joint surface; osteoporosis weakens the bone structure
- OA causes direct knee joint pain; osteoporosis creates fracture risk
- OA is treated with joint care, injections, and replacement if needed; osteoporosis is treated with calcium, Vitamin D, and bone-strengthening medications
When both conditions coexist – which is common in older women – both must be diagnosed and treated together.
How to Prevent Arthritis in the Knees
Not all knee arthritis can be prevented, especially when genetics or autoimmune factors are involved. However, these practical steps can significantly reduce your risk or delay the onset:
- Maintain a healthy body weight: This is the single most impactful preventive measure. Every extra kilogram adds approximately 4 to 5 kg of load on each knee joint with every step you take.
- Stay physically active: Low-impact exercise – walking, swimming, cycling, yoga – keeps the muscles around the knee strong and the cartilage healthy. A strong knee is a more protected knee.
- Protect your knees from injury: Use proper technique during sport and exercise. Wear supportive footwear. Avoid prolonged kneeling or deep squatting whenever possible.
- Treat knee injuries promptly: Meniscal tears and ligament injuries that are left untreated accelerate posttraumatic arthritis significantly. Early treatment makes a lasting difference.
- Quit smoking: Smoking is a recognised risk factor for rheumatoid arthritis and impairs tissue healing throughout the body.
- Focus on diet and nutrition: An anti-inflammatory diet rich in omega-3 fatty acids, fruits, vegetables, and whole grains supports joint health over the long term. Adequate Vitamin D and calcium intake protect the bone beneath the cartilage as well.
Conclusion
Knee arthritis – whether it is OA knee, rheumatoid arthritis in the knees, or posttraumatic arthritis – is not something you simply have to endure. Modern orthopaedic care offers a full range of solutions, from early lifestyle changes to the most advanced surgical techniques available today.
The most important step is getting an accurate diagnosis early. The stage of your arthritis determines the best treatment path – and the earlier you act, the more options you have.
At deformity.co.in, our specialists combine precision diagnosis with compassionate, personalised care – because you deserve to walk without pain.
Key Takeaways:
- Knee arthritis means cartilage breakdown, causing pain, swelling, and stiffness in the knee joint
- The three main types are Osteoarthritis (OA knee), Rheumatoid Arthritis (RA in knees), and Posttraumatic Arthritis
- Early symptoms include morning stiffness, swelling, crepitus, and pain during or after activity
- Diagnosis uses physical examination, arthritic knee X-ray, MRI, and blood tests
- Non-surgical care – physiotherapy, weight loss, NSAIDs, injections – is always the first step
- Surgery, including osteotomy, partial or total knee replacement, is reserved for advanced cases
- Bilateral knee OA is very common in India and highly treatable
- Early action gives you the most options and the best outcomes
FAQs
What is meant by arthritis in the knee?
Knee arthritis means the cartilage covering the knee joint has broken down, causing bones to rub together. This leads to pain, swelling, stiffness, and reduced movement in the knee joint over time.
What is the OA knee full form?
OA knee stands for Osteoarthritis of the Knee – the most common type of knee arthritis, caused by gradual wear and degeneration of cartilage inside the knee joint over many years.
What are the early symptoms of arthritis in the knees?
Early signs include morning stiffness, mild swelling, pain after physical activity, and a creaking or clicking sensation in the knee. Pain typically eases with rest in the early stages of OA knee.
What causes knee joint pain and swelling?
In arthritis, the joint produces excess fluid in response to inflammation. This causes characteristic swelling alongside knee joint pain that worsens progressively during and after physical activity.
What is bilateral knee osteoarthritis?
Bilateral knee osteoarthritis means OA affects both the left and right knees simultaneously. It is common in older Indian adults and may require staged or simultaneous treatment for both knee joints.
What is the best treatment for osteoarthritis in the knees?
Treatment depends on severity. Mild-to-moderate OA is managed with physiotherapy, weight loss, NSAIDs, and injections. An advanced OA knee may require partial or total knee replacement surgery for lasting relief.
How is knee arthritis different from osteoporosis of the knee?
Knee arthritis is cartilage degeneration, causing direct joint pain. Osteoporosis is reduced bone density that increases fracture risk. They are different conditions, but can coexist in older patients simultaneously.
What is tricompartmental osteoarthritis?
Tricompartmental OA means arthritis has damaged all three compartments of the knee – medial, lateral, and patellofemoral. It represents advanced disease and is commonly treated with total knee replacement surgery.
What is the difference between rheumatoid arthritis and OA of the knee?
OA is mechanical wear-and-tear of cartilage, most common in older adults. RA is autoimmune – the immune system attacks the joint lining – and typically affects both knees symmetrically, often in younger patients.
Can knee arthritis be cured permanently?
There is no permanent cure for arthritis. However, with the right treatment – physiotherapy, medication, or surgery – most patients achieve significant pain relief and can restore a comfortable, functional daily life.