Breaking your thighbone is one of the most serious fractures you can experience. If you or a loved one has suffered a femur fracture, you’re likely facing questions about treatment, surgery, and the road to recovery. This comprehensive guide will walk you through everything you need to know about femoral shaft fractures, from initial symptoms to complete rehabilitation.
Understanding what lies ahead can reduce anxiety and help you prepare for the healing journey. While a broken femur is undoubtedly a significant injury, modern surgical techniques and rehabilitation protocols have made recovery more predictable and successful than ever before.
What is a Femur Shaft Fracture?
A femur shaft fracture refers to a break in the long, central portion of your thighbone. The femur is the largest and strongest bone in the human body, extending from your hip to your knee. When we talk about the “shaft,” we’re referring to the long, straight section in the middle of this bone, excluding the rounded ends near the hip and knee joints.
Understanding Your Thigh Bone Anatomy
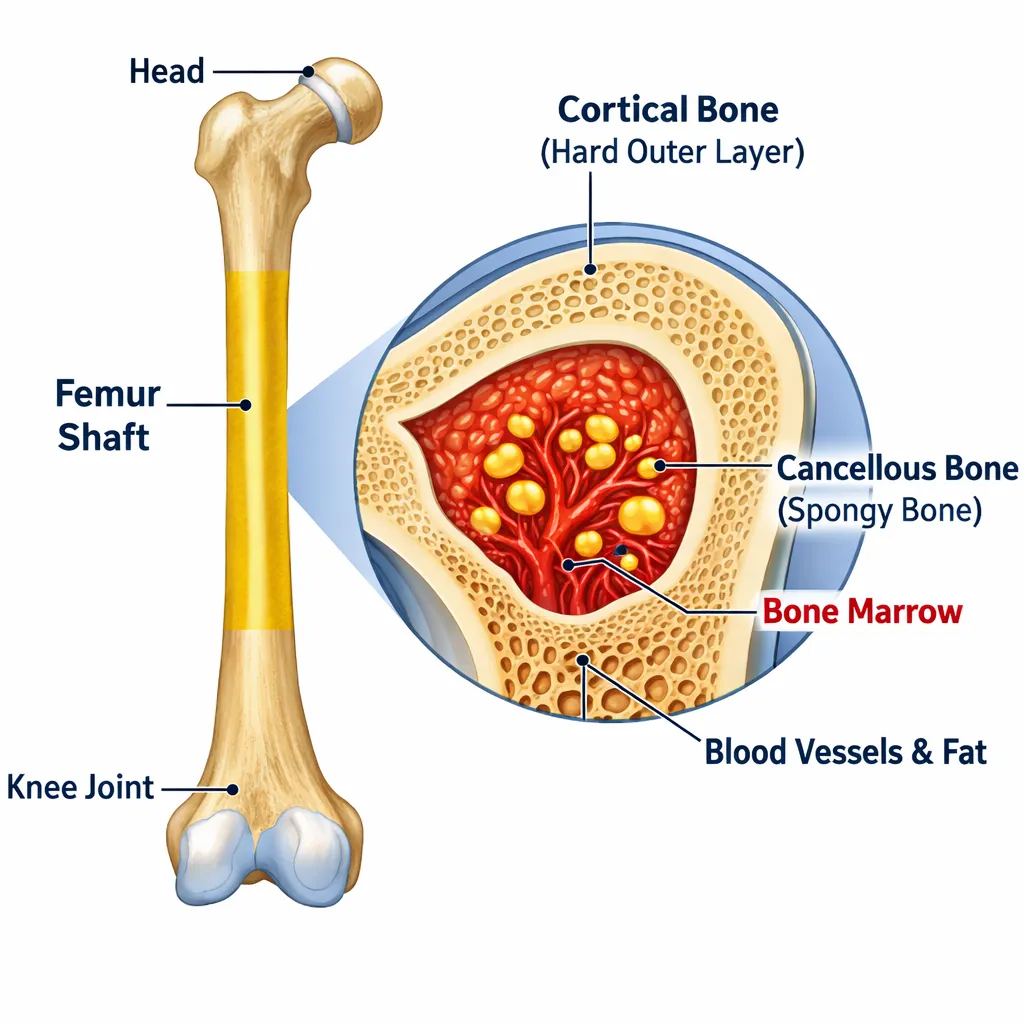
Your femur plays a critical role in supporting your body weight and enabling movement. This impressive bone can withstand tremendous pressure during normal activities like walking, running, and jumping. The shaft portion is particularly strong because it’s designed to bear and distribute forces throughout your leg.
The bone itself consists of a hard outer layer called cortical bone and a softer inner section containing bone marrow. This structure provides both strength and flexibility, allowing your femur to handle stress without breaking under normal circumstances.
Why Femur Fractures Are Considered Serious
Because the femur is so robust, it takes significant force to cause a fracture. This means that when a femoral shaft fracture occurs, it’s often accompanied by other injuries. Additionally, the femur is surrounded by major blood vessels and muscles, making complications more likely if not treated promptly.
The location of your thigh bone in the body means that a fracture here affects your entire leg’s stability and function. Unlike smaller bone fractures that might heal with simple immobilization, a broken thighbone almost always requires surgical intervention to ensure proper healing and alignment.
Common Causes of Femur Bone Fractures
Understanding how femur fractures occur can provide context for your injury and help with prevention in the future.
High-Impact Injuries in Young Adults
For younger individuals with healthy bones, femur fractures typically result from high-energy trauma. Motor vehicle accidents are the leading cause, especially when the knee impacts the dashboard during a collision. The force travels up through the leg, causing the femoral shaft to break.
Motorcycle accidents present similar risks, often resulting in more severe fracture patterns due to the lack of protective barriers. Other common causes include:
- Falls from significant heights (construction sites, ladders, roofs)
- Pedestrian accidents when struck by vehicles
- Sports injuries in high-impact activities
- Industrial accidents involving heavy machinery
In these scenarios, the tremendous force overcomes the femur’s natural strength, causing it to snap or shatter.
Low-Impact Fractures in Older Adults
For elderly individuals, particularly those with osteoporosis or weakened bones, a femur fracture can occur from much less force. A simple fall from standing height or even a minor stumble can be enough to break the thigh bone when bone density has decreased significantly.
This type of fracture is concerning because it indicates bone fragility and increases the risk of future fractures. If you’re over 65 and have experienced a femur fracture from a minor fall, your doctor will likely recommend a bone density evaluation.
Types of Femoral Shaft Fractures
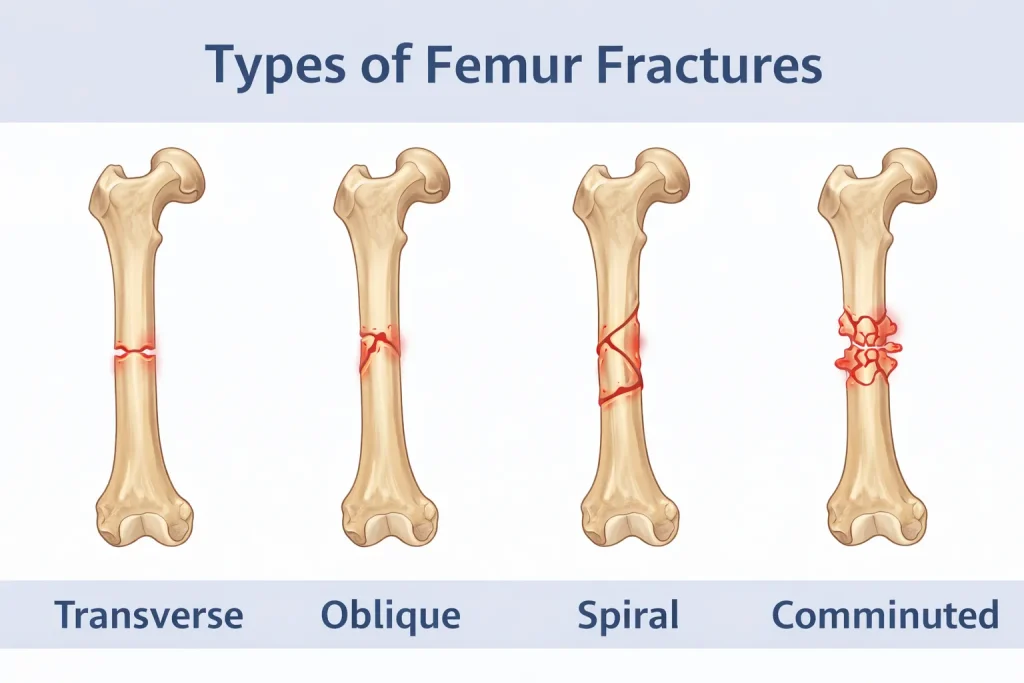
Not all femur fractures are the same. Doctors classify these injuries based on the pattern of the break, which influences treatment decisions and recovery expectations.
Transverse Fracture
A transverse fracture creates a straight, horizontal break line across the bone shaft. Imagine snapping a pencil in half-that’s essentially what a transverse fracture looks like. This pattern typically results from a direct blow to the thigh or a bending force applied to the leg.
These fractures are generally considered more stable than other types because the break line is perpendicular to the bone’s length, making it easier for surgeons to realign and secure the fragments.
Oblique and Spiral Fractures
An oblique fracture features an angled break line across the shaft, while a spiral fracture winds around the bone like a barber pole stripe. Spiral fractures specifically occur when a twisting force is applied to the leg, such as when your foot is planted but your body rotates.
These fracture patterns can be more challenging to stabilize because the angled break creates surfaces that may slip past each other if not properly secured during healing.
Comminuted Fracture
A comminuted femur fracture is one of the most severe types, involving the bone breaking into three or more separate pieces. These injuries typically result from extremely high-energy impacts and often accompany other serious trauma.
Comminuted fractures require meticulous surgical technique to realign all the fragments and achieve stable fixation. Recovery time is generally longer, and the risk of complications increases with the complexity of the fracture pattern.
Open vs. Closed Fractures
This classification refers to whether the skin remains intact. In a closed fracture, the broken bone doesn’t penetrate the skin’s surface. An open fracture (also called a compound fracture) occurs when bone fragments break through the skin or when an external wound reaches down to the fracture site.
Open fractures carry a significantly higher risk of infection because the bone is exposed to bacteria from the environment. These injuries require immediate surgical cleaning and typically need antibiotics to prevent serious complications.
Femur Fracture Symptoms: Recognizing the Signs
Identifying a femur fracture is usually straightforward because the symptoms are dramatic and unmistakable.
Immediate Warning Signs
The moment a femur shaft fracture occurs, you’ll experience:
Severe, immediate pain – This is typically described as the worst pain the person has ever felt. The pain is localized to the thigh but may radiate throughout the leg.
Complete inability to stand or bear weight – Unlike some fractures, where you might be able to limp, a broken femur makes standing impossible. The leg cannot support any body weight.
Visible deformity – The injured leg may appear shorter than the uninjured leg, and you might notice an abnormal angle or position that looks clearly wrong. The thigh may appear twisted or bent unnaturally.
Swelling and bruising – The thigh will begin swelling rapidly, and extensive bruising typically develops within hours as blood vessels around the fracture site are damaged.
Inability to move the leg – Any attempt to move the leg at the hip or knee causes excruciating pain, and the leg may feel unstable or like it’s “disconnected.”
Can You Walk on a Fractured Leg?
This is one of the most common questions people ask after a leg injury. With a femur shaft fracture, the answer is definitely no. The structural integrity of your leg is completely compromised, making weight-bearing impossible and potentially dangerous.
Attempting to walk on a broken femur could:
- Worsen the fracture by causing further displacement
- Damage to the surrounding blood vessels and nerves
- Transform a closed fracture into an open one
- Causes severe additional pain
If you suspect a femur fracture, don’t attempt to move the leg. Call for emergency medical help immediately and keep the leg as still as possible while waiting for assistance.
Diagnosis: How Doctors Identify Femur Fractures
When you arrive at the emergency room with a suspected thigh bone fracture, medical professionals follow a systematic approach to confirm the diagnosis and assess the injury’s severity.
Physical Examination
Before ordering imaging tests, your doctor will conduct a thorough physical assessment. They’ll ask detailed questions about:
- How the injury occurred (mechanism of injury)
- Whether you heard or felt a “pop” or “snap.”
- Your medical history and current medications
- Any allergies you have
- Whether you use tobacco products (this affects healing)
The physical exam involves carefully inspecting your injured leg without causing unnecessary movement. Your doctor will check for:
- Obvious deformities or abnormal positioning
- Open wounds or skin breaks
- Areas of severe bruising or swelling
- Pulses in your foot to ensure blood flow
- Sensation in your leg and foot to check nerve function
- The tension of skin and muscles (to assess for compartment syndrome)
This examination helps doctors understand not just the fracture itself but also whether any complications like nerve damage or vascular injury have occurred.
Imaging Tests and X-Rays

X-rays are the primary diagnostic tool for confirming a femur fracture. Technicians will take images from multiple angles-typically front-to-back and side views-to fully visualize the break.
X-rays clearly show:
- The exact location of the fracture along the shaft
- The fracture pattern (transverse, oblique, spiral, or comminuted)
- How displaced the bone fragments are
- Whether the break extends into nearby joints
CT scans may be ordered if:
- The X-ray shows a complex fracture pattern that needs better visualization
- Doctors suspect the fracture extends into the hip or knee joint
- Very thin fracture lines are difficult to see on standard X-rays
- Surgical planning requires detailed three-dimensional imaging
CT scans provide cross-sectional images that help surgeons plan the best approach for your specific injury.
Femur Fracture Treatment Options
The vast majority of femur shaft fractures require surgery. Unlike arm or hand fractures that might be treated with casts alone, the thigh bone needs internal support to heal properly.
Emergency Stabilization
Before definitive surgery can be performed, emergency room doctors focus on stabilizing your condition. This involves:
Pain management – Powerful pain medications are administered to keep you comfortable while tests and preparations proceed.
Temporary immobilization – Your leg may be placed in a long-leg splint or special device to prevent further movement and damage.
Skeletal traction – In some cases, doctors apply traction, which uses weights and pulleys to gently pull the leg into better alignment. This reduces pain and maintains leg length until surgery.
Monitoring – Medical staff will continuously check your leg’s circulation, sensation, and muscle tension to catch any developing complications early.
Most femur fractures are repaired surgically within 24 to 48 hours of injury. However, if you have other life-threatening injuries, surgery may be delayed until you’re medically stable.
Surgical Treatment Methods
Modern orthopedic surgery offers several techniques for fixing femoral shaft fractures. Your surgeon chooses the best method based on your fracture pattern, age, overall health, and other factors.
Intramedullary Nailing Procedure
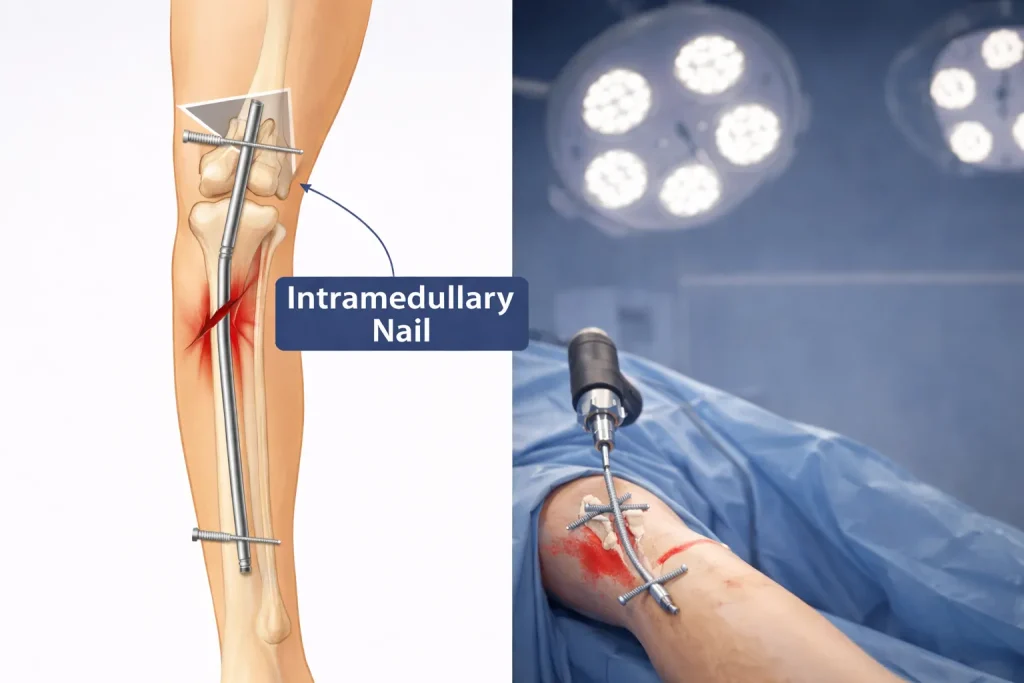
Intramedullary nailing has become the gold standard for treating most femur shaft fractures. This technique involves inserting a metal rod directly into the hollow center (medullary canal) of your femur.
Here’s how the procedure works:
Access – The surgeon makes a small incision, either near your hip or knee, to access the femur’s canal.
Rod insertion – A specially designed titanium rod is carefully guided through the center of your femur, crossing the fracture site. The rod acts as an internal splint, holding the bone in proper alignment.
Screw placement – Metal screws are inserted through the bone and rod both above and below the fracture. These screws, called “locking screws,” prevent the rod from rotating and keep your leg at the correct length.
Closure – The incisions are closed, and your leg is bandaged.
The major advantages of intramedullary nailing include:
- Provides strong, stable fixation throughout the bone’s length
- Allows early movement and weight-bearing in many cases
- Smaller incisions mean less tissue damage
- The rod remains inside permanently (unless complications develop)
External Fixation
External fixation uses metal pins or screws that pass through the skin and into the bone above and below the fracture. These pins connect to a rigid external frame that holds everything in position.
External fixators are typically used when:
- Extensive soft tissue damage makes immediate internal surgery risky
- You have multiple injuries requiring staged treatment
- Severe swelling or open wounds need to heal before definitive surgery
- The fracture is part of a complex trauma with vascular injury
External fixators provide good temporary stability and can be adjusted as needed. However, they’re usually replaced with internal fixation (like a rod) once your condition stabilizes. In rare cases, the external fixator remains in place throughout the entire healing process.
Plates and Screws
For certain fracture patterns-particularly those extending into the hip or knee joints-surgeons may use plates and screws instead of intramedullary rods. This technique involves:
Open reduction – Making an incision along the thigh to directly expose the fracture site.
Realignment – Carefully repositioning the bone fragments into anatomic alignment.
Plate application – Attaching a specially contoured metal plate to the outer surface of the bone with multiple screws.
While this method requires a larger incision and more tissue disruption, it provides excellent fracture visualization and precise positioning for complex breaks.
Femur Fracture Recovery Time: What to Expect

One of the first questions patients ask is, “How long until I’m healed?” Recovery from a femur fracture is measured in months, not weeks, but understanding the timeline helps you set realistic expectations.
Typical Healing Timeline
Initial healing phase (6-8 weeks) – During the first two months, new bone begins forming at the fracture site. You’ll notice pain gradually decreasing, though the bone is still fragile.
Consolidation phase (3-4 months) – The new bone becomes denser and stronger. Most patients experience significant improvement in comfort and function during this period.
Remodeling phase (6-12 months) – The bone continues strengthening and reshaping itself. While you may return to normal activities during this time, the bone is still remodeling internally.
Complete healing – Most femur shaft fractures achieve complete healing within 3 to 6 months. However, more complex fractures may take 9 to 12 months for full recovery.
Factors Affecting Recovery Speed
Several factors influence how quickly your femur heals:
Fracture severity – Simple transverse fractures heal faster than comminuted fractures with multiple fragments.
Age – Younger patients typically heal more quickly due to more active bone metabolism.
Tobacco use – Smoking significantly delays bone healing and increases complication risks. Quitting smoking before and after surgery dramatically improves outcomes.
Nutrition – Adequate protein, calcium, and vitamin D intake supports bone formation.
Compliance – Following weight-bearing restrictions and physical therapy recommendations accelerates recovery.
Overall health – Conditions like diabetes or poor circulation can slow healing.
Rehabilitation and Physical Therapy

Physical therapy is essential for regaining strength, mobility, and function after a femur fracture. Your rehabilitation journey typically begins while you’re still in the hospital.
Early Mobility Exercises
Even before you leave the hospital, physical therapists will teach you:
Ankle pumps – Moving your foot up and down to prevent blood clots and maintain circulation.
Quadriceps sets – Tightening your thigh muscles to prevent atrophy (muscle wasting).
Hip and knee range-of-motion exercises – Gentle movements to maintain joint flexibility.
Transfer training – Safe techniques for getting in and out of bed, chairs, and using the bathroom.
Crutch walking – Proper use of assistive devices for safe mobility.
These early exercises might seem simple, but they’re crucial for preventing complications and preparing your leg for more advanced rehabilitation.
Weight-Bearing Progression
Your surgeon will provide specific instructions about how much weight you can put on your injured leg. Common protocols include:
Non-weight-bearing – Keeping all weight off the injured leg, using crutches or a walker.
Toe-touch weight-bearing – Touching your toes to the floor for balance only.
Partial weight-bearing – Gradually increasing weight, often progressing from 25% to 50% to 75% of your body weight.
Weight-bearing as tolerated – Putting as much weight as you’re comfortable with, guided by pain levels.
Full weight-bearing – Walking normally without restrictions.
Many modern surgical techniques allow patients to bear weight relatively early in recovery, but always follow your surgeon’s specific guidelines. Putting too much weight too soon can displace the fracture or damage the surgical hardware.
Returning to Normal Activities
Returning to work and daily activities follows a gradual progression:
4-6 weeks – Light desk work may be possible if you can commute safely.
8-12 weeks – Most patients can perform basic daily activities independently.
3-4 months – Return to physical jobs may be cleared, depending on demands.
6-9 months – High-impact activities and sports can typically resume with surgeon approval.
Always communicate with your surgeon before increasing activity levels, especially for demanding physical work or recreational sports.
Potential Complications of Femur Fractures
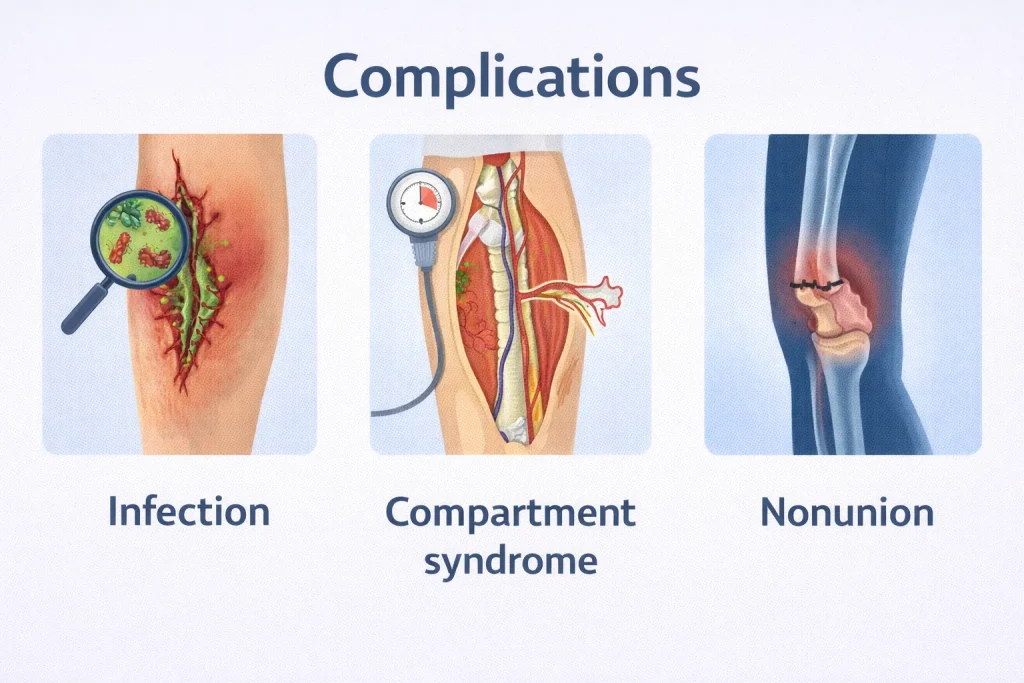
While most femur fractures heal successfully, being aware of potential complications helps you recognize problems early.
Infection Risks
Superficial infections around incision sites cause redness, warmth, and drainage but respond well to antibiotics.
Deep bone infections (osteomyelitis) are more serious, potentially requiring additional surgery to clean the bone. Open fractures carry the highest infection risk.
Signs of infection include:
- Increasing pain after initial improvement
- Fever and chills
- Wound drainage with foul odor
- Redness spreading from the incision
- Warmth over the fracture site
Contact your surgeon immediately if you notice these symptoms.
Compartment Syndrome
Compartment syndrome is a surgical emergency that can develop when pressure builds up inside the muscle compartments of your thigh. This pressure reduces blood flow, potentially causing permanent muscle and nerve damage.
Warning signs include:
- Pain that seems out of proportion to the injury
- Pain that worsens with passive stretching
- Numbness or tingling in the foot
- Pale or cool skin on the leg
- Tight, swollen thigh that feels hard
If diagnosed, emergency surgery to release the pressure is necessary to prevent permanent damage.
Nonunion and Delayed Healing
Most femur fractures heal predictably, but sometimes the bone fails to unite properly. Delayed union means healing is progressing, but slower than expected. Nonunion occurs when the bone stops healing entirely, leaving a gap that won’t close without additional treatment.
Risk factors include:
- Severe initial injury with significant bone loss
- Inadequate blood supply to the fracture site
- Infection
- Tobacco use
- Poor nutrition
- Certain medications
Treatment for nonunion typically requires another surgery, possibly including bone grafting to stimulate healing.
Pain Management After Femur Surgery
Controlling pain is essential for both comfort and recovery, as adequate pain relief allows you to participate in physical therapy more effectively.
Medication Options
Your pain management plan may include:
Acetaminophen – Over-the-counter pain reliever that’s safe for most patients.
NSAIDs – Anti-inflammatory medications like ibuprofen help reduce pain and swelling.
Opioid medications – Strong prescription pain relievers used immediately after surgery, then tapered as pain improves.
Nerve pain medications – Gabapentin or similar drugs for nerve-related discomfort.
Muscle relaxants – To ease muscle spasms that commonly occur around fractures.
Your doctor will carefully balance pain relief with minimizing medication side effects and dependency risks.
Alternative Pain Relief Methods
Non-medication approaches that can help include:
Ice therapy – Applied to the thigh for 15-20 minutes several times daily.
Elevation – Keeping your leg elevated reduces swelling and associated pain.
Gentle movement – Paradoxically, appropriate exercises often reduce pain by preventing stiffness.
Relaxation techniques – Deep breathing, meditation, and visualization can help manage pain perception.
Long-Term Outlook and Prevention
The good news is that most people who suffer femur shaft fractures make excellent recoveries. With modern surgical techniques and committed rehabilitation, you can expect to return to your previous activity level.
Long-term function – Studies show that 80-90% of patients regain full or near-full function within one year of injury.
Hardware removal – The intramedullary rod and screws typically remain in place permanently unless they cause problems. Removal is a personal choice discussed with your surgeon.
Preventing future fractures involves:
- Bone density screening if you’re over 50
- Fall prevention strategies for older adults
- Proper nutrition with adequate calcium and vitamin D
- Regular weight-bearing exercise to maintain bone strength
- Avoiding tobacco products
- Safe driving practices
- Using appropriate safety equipment during sports and work
Remember that healing is a journey. Be patient with yourself, celebrate small victories, and maintain open communication with your healthcare team. With time and dedication to your recovery plan, you can overcome a femur fracture and return to the life you love.
Conclusion
Femur shaft fractures – a break in the strongest bone in your body – represent a serious injury, but the outlook is genuinely positive with modern surgical techniques and dedicated rehabilitation.
Key takeaways from this article:
- Surgery is essential – intramedullary nailing provides stable fixation for reliable healing
- Expect 3-6 months for complete recovery – healing takes time, with gradual progress throughout
- Physical therapy is critical – consistent rehabilitation restores strength and normal walking
- Watch for warning signs – increasing pain, fever, or numbness requires immediate medical attention
- Quit smoking – tobacco dramatically slows healing and increases complications
- Follow weight-bearing rules – protecting your fracture prevents hardware failure
- Full recovery is achievable – 80-90% of patients return to previous activity levels
Understanding your injury empowers you to participate actively in recovery. Work closely with your surgical team, stay committed to rehabilitation, follow medical guidance carefully, and give your bone the time it needs to heal. Your dedication today builds the foundation for complete recovery tomorrow.
FAQs
How long does it take to walk again after a femur fracture?
Most patients begin walking with crutches or a walker within days after surgery. Independent walking typically takes 6-12 weeks, depending on your healing progress and surgeon’s protocol. Normal walking without limping usually returns within 3-6 months.
Can a femur fracture heal without surgery?
No, nearly all adult femur shaft fractures require surgery. The femur is a weight-bearing bone that needs strong internal fixation to heal properly aligned. Without surgery, the bone would heal shortened, deformed, or not at all.
What is the most painful bone to break?
The femur is considered one of the most painful bones to break due to its size, surrounding muscle tissue, and the severe trauma required to fracture it. Patients consistently describe the pain as debilitating, making standing impossible.
Will I have a limp after femur fracture surgery?
Most patients do not develop a permanent limp with proper healing and diligent physical therapy. Temporary limping is common during recovery while rebuilding strength. Persistent limping beyond 6-9 months requires additional evaluation.
What are the signs my femur fracture isn’t healing properly?
Warning signs include persistent or increasing pain after 6-8 weeks, inability to progress with weight-bearing, visible deformity, fever, infection signs, or X-rays showing no new bone formation. Contact your surgeon immediately if these occur.