The Weber Classification of Ankle Fracture is one of the most widely used systems to categorize ankle fractures. It classifies distal fibula fractures based on their level relative to the syndesmosis – the ligament complex that connects the tibia and fibula. This simple but powerful system helps doctors determine fracture stability, the need for surgery, and expected recovery time.
In this comprehensive guide, you will learn:
Table of Contents
What is Weber Classification?
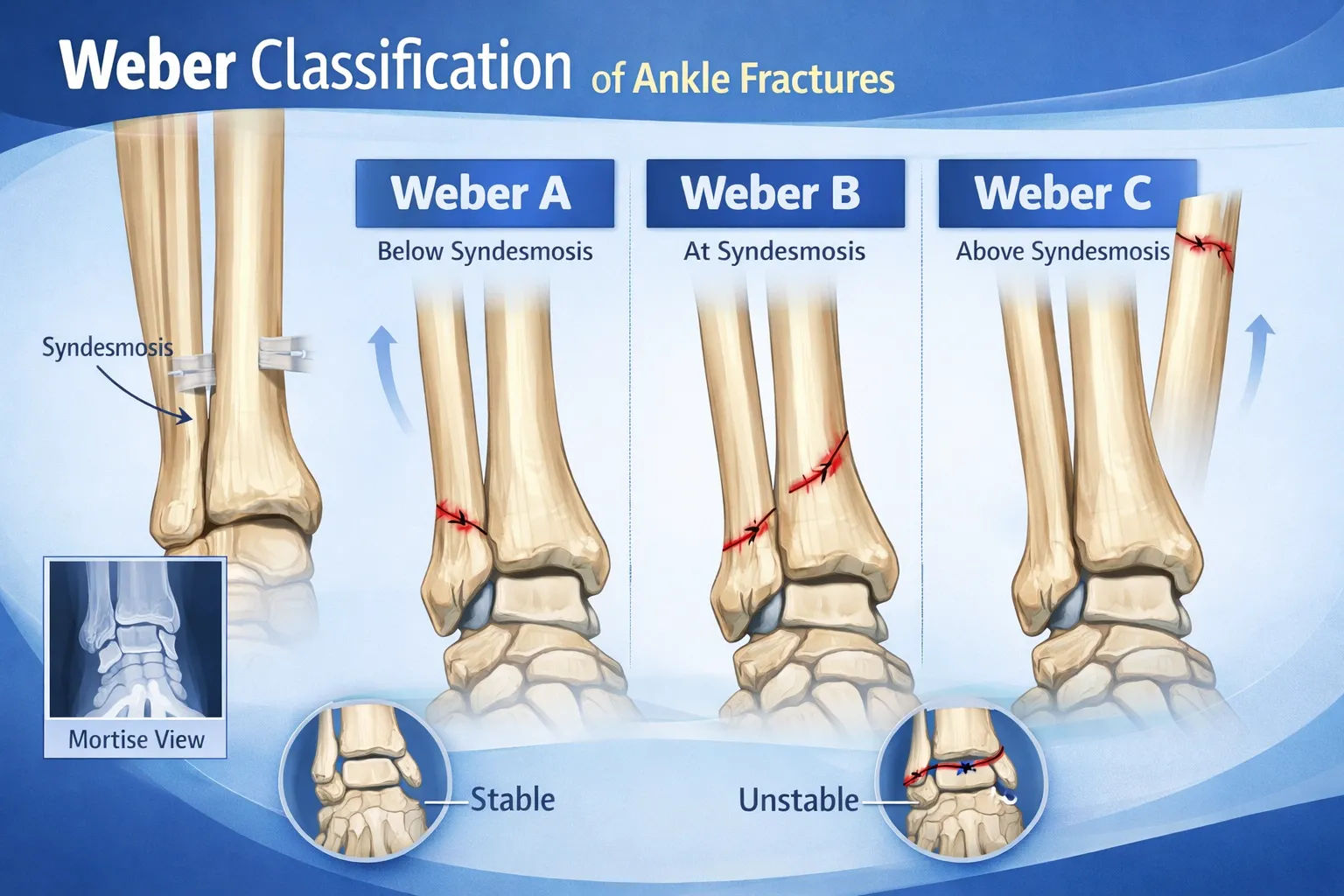
The Weber classification system categorizes ankle fractures based on the location of the fibular fracture relative to the syndesmosis.
It divides fractures into three types:
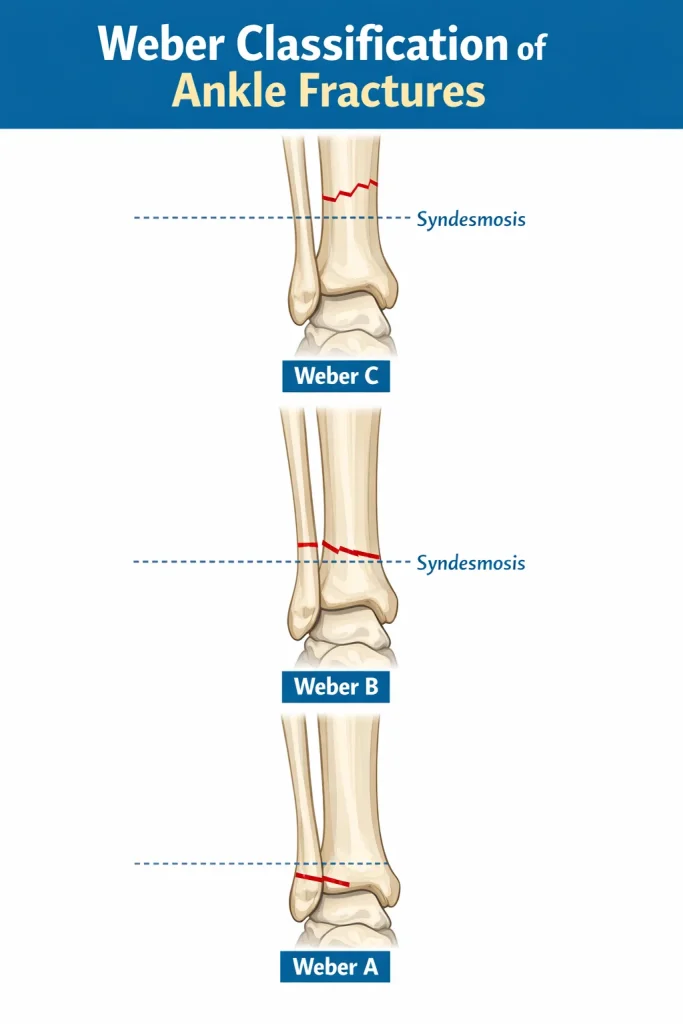
- Weber A – fracture below the syndesmosis
- Weber B – fracture at the level of the syndesmosis
- Weber C – fracture above the syndesmosis
The higher the fracture, the greater the likelihood of syndesmotic injury and ankle instability.
Key concepts:
- Focuses on the distal fibula fracture
- Assesses stability indirectly
- Guides treatment decisions
- Used globally in orthopedic practice
Because ankle stability determines treatment, the Weber classification remains clinically important worldwide.
History of the Weber Classification: Danis-Weber System
The Weber classification was originally developed by Swiss surgeon Robert Danis in 1949 and later refined by Bernhard Georg Weber in 1966. This is why you will often see it referred to as the Danis-Weber classification in academic literature.
Weber adapted Danis’s original work to create the three-tier A, B, C system that orthopedic surgeons use today. The system was further expanded by Weber and Cech to include a 4th type in some academic contexts, though clinical practice universally focuses on Types A, B, and C.
Why it became the global standard:
- Simple to apply on plain X-ray
- Directly correlates with treatment decisions
- Reproducible across different centers and countries
- Aligns with syndesmotic anatomy
The Danis-Weber classification remains the most commonly cited ankle fracture system in orthopedic textbooks and surgical planning worldwide.
History of the Weber Classification: Danis-Weber System
The Weber classification was originally developed by Swiss surgeon Robert Danis in 1949 and later refined by Bernhard Georg Weber in 1966. This is why you will often see it referred to as the Danis-Weber classification in academic literature.
Weber adapted Danis’s original work to create the three-tier A, B, C system that orthopedic surgeons use today. The system was further expanded by Weber and Cech to include a 4th type in some academic contexts, though clinical practice universally focuses on Types A, B, and C.
Why it became the global standard:
- Simple to apply on plain X-ray
- Directly correlates with treatment decisions
- Reproducible across different centers and countries
- Aligns with syndesmotic anatomy
The Danis-Weber classification remains the most commonly cited ankle fracture system in orthopedic textbooks and surgical planning worldwide.
Understanding the Syndesmosis
The syndesmosis is a ligament complex that connects the distal tibia and fibula. It maintains alignment of the ankle mortise and prevents separation of the two bones during weight-bearing.
Important structures include:
- Anterior inferior tibiofibular ligament
- Posterior inferior tibiofibular ligament
- Interosseous ligament
Functions of the syndesmosis:
- Stabilizes the ankle joint
- Maintains mortise integrity
- Prevents talar shift
- Supports walking mechanics
In Weber B and C fractures, syndesmotic injury may occur, leading to instability that often requires surgical fixation.
Weber A Fracture

A Weber A fracture occurs below the level of the syndesmosis. These fractures are typically stable because the syndesmotic ligaments remain intact.
Radiology Findings
- Fracture line below the ankle joint
- Syndesmosis intact
- No talar shift
Treatment
- Walking boot or cast
- Rest and elevation
- Pain management
- Gradual weight-bearing
Most Weber A fractures heal without surgery and have good outcomes.
Weber B Fracture

A Weber B fracture occurs at the level of the syndesmosis. This is the most common Weber type. Stability varies depending on ligament involvement.
Radiology Features
- Oblique fracture line
- Fracture at the joint level
- Possible medial malleolus involvement
When Surgery Is Needed
Surgery may be required if:
- Talar shift is present
- The medial clear space is widened
- Syndesmotic injury exists
- Fracture is displaced
Weber B fractures require careful assessment because some are stable while others are unstable.
Stable vs Unstable Weber B Fracture
This is the most critical distinction in Weber B management, and it is what every treating surgeon must determine before choosing between conservative and surgical care.
Stable Weber B fracture:
- Syndesmosis remains intact
- No widening of the medial clear space
- No talar shift on stress X-ray
- The deltoid ligament is uninjured
- Can be treated with a cast or boot
Unstable Weber B fracture:
- Syndesmosis is disrupted
- Medial clear space widened (>4 mm on mortise view)
- Talar shift present
- The deltoid ligament may be torn
- Requires surgical fixation
The gravity stress test, or external rotation stress X-ray, is routinely used to assess stability in borderline Weber B cases. If talar shift appears under stress, the fracture is considered unstable, and surgery is recommended.
Weber B Fracture with Talar Shift
Talar shift is a key radiological finding that changes management. When the talus shifts laterally within the ankle mortise, it indicates the medial structures have been compromised. Even a 1 mm lateral shift of the talus significantly reduces the ankle joint contact area, increasing the long-term risk of post-traumatic arthritis.
A Weber B fracture with talar shift should be treated surgically to restore the ankle mortise to its normal alignment.
Weber C Fracture

A Weber C fracture occurs above the syndesmosis. These fractures are usually unstable and associated with ligament disruption.
Radiology Features
- High fibular fracture
- Widened ankle mortise
- Syndesmotic separation
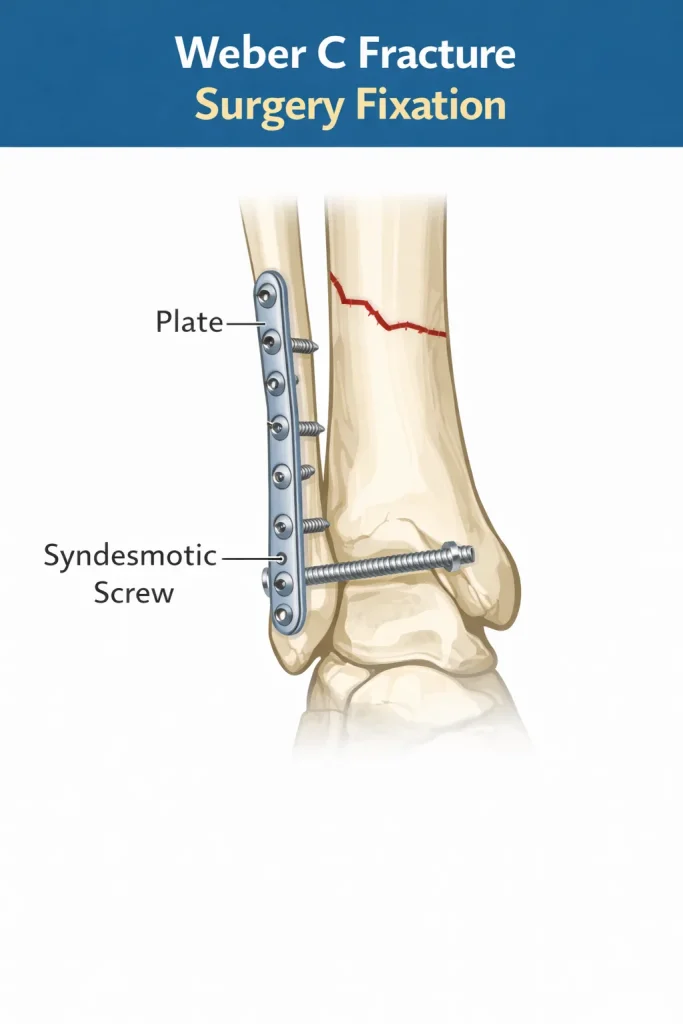
Surgical Management
Most Weber C fractures require:
- Plate fixation of the fibula
- Syndesmotic screw or tightrope fixation
- Restoration of ankle alignment
Because the syndesmosis is disrupted, surgical stabilization is commonly required.
The goal of surgery is to restore the normal relationship between the tibia, fibula, and talus – known as the ankle mortise. When the mortise is not properly restored, long-term outcomes deteriorate significantly.
Surgical steps for Weber C fracture:
- Open reduction of the fibular fracture
- Internal fixation with a plate and screws
- Assessment of syndesmotic stability intraoperatively
- Syndesmotic fixation if instability is confirmed (screw or suture button/tightrope)
- Assessment of the medial side if deltoid ligament is torn
Weber C fracture conservative treatment:
In rare cases – such as frail elderly patients with significant comorbidities who cannot tolerate surgery – conservative management with a non-weight-bearing cast may be considered. However, this is the exception rather than the rule. Without surgical stabilization, the risk of malunion and progressive ankle arthritis is considerably higher in Weber C injuries.
Is a Weber C Fracture Serious?
Yes. Weber C fractures are the most serious of the three types. They involve ligament disruption above the syndesmosis, which means the ankle joint loses its structural integrity. Without proper treatment, patients risk:
- Chronic ankle instability
- Progressive deformity
- Early post-traumatic arthritis
- Significant loss of function
Early surgical intervention and proper rehabilitation are critical to achieving a good outcome.
Weber Classification Comparison Table
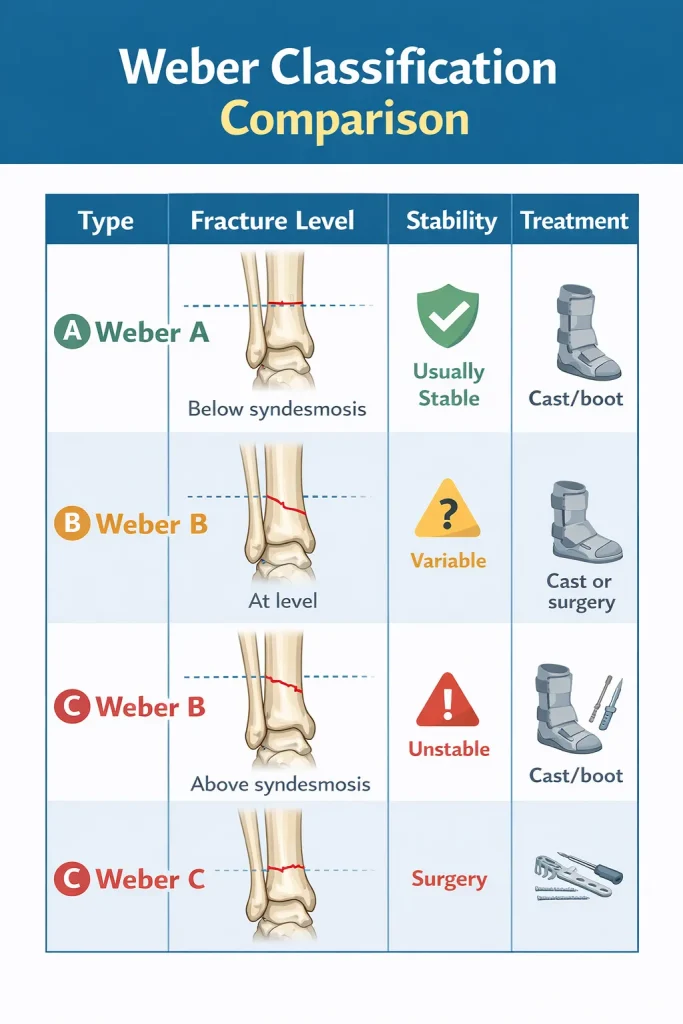
| Type | Fracture Level | Stability | Treatment |
|---|---|---|---|
| Weber A | Below syndesmosis | Usually stable | Cast/boot |
| Weber B | At level | Variable | Cast or surgery |
| Weber C | Above syndesmosis | Unstable | Surgery |
This classification helps guide management and prognosis.
Weber Classification and Ankle Stability
Ankle stability depends on whether the syndesmosis remains intact.
- Weber A – stable because the syndesmosis is intact
- Weber B – may or may not involve syndesmosis
- Weber C – usually unstable due to ligament disruption
Instability increases the risk of arthritis if untreated. Therefore, accurate classification is essential.
Weber vs Lauge-Hansen Classification
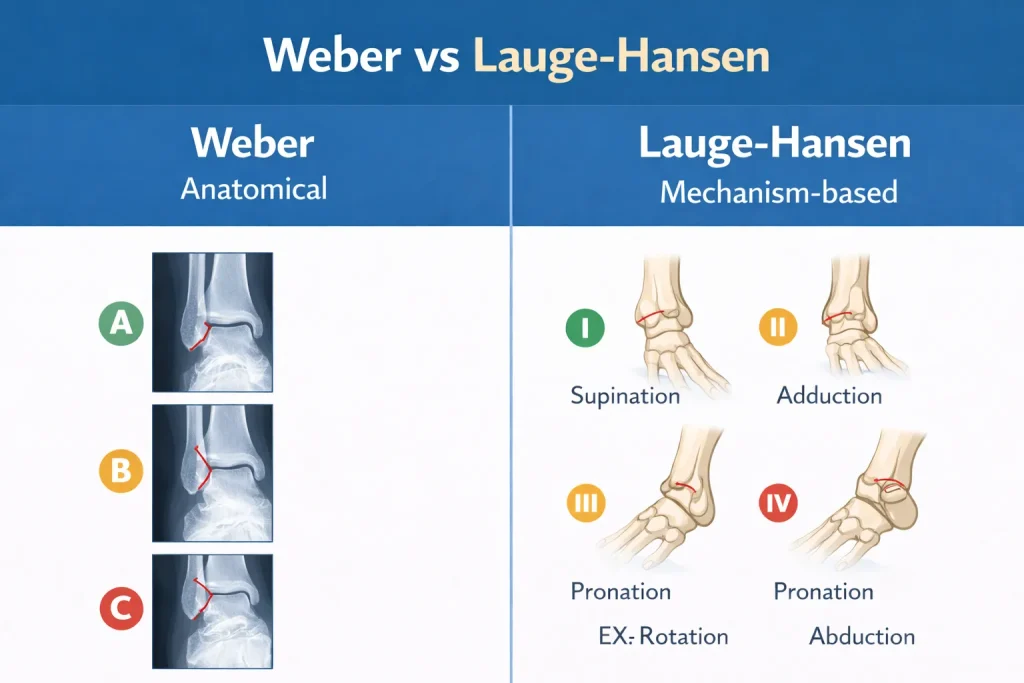
The Weber classification is anatomical, focusing on fracture level.
The Lauge-Hansen classification is mechanism-based, describing how the injury occurred.
Comparison:
- Weber → simple and practical
- Lauge-Hansen → detailed but complex
- Weber is widely used in clinical practice
Both systems are valuable, but Weber remains easier for everyday decision-making.
How Lauge-Hansen Relates to Weber Types
The Lauge-Hansen system describes four injury patterns based on foot position and the direction of applied force at the time of injury:
- Supination-Adduction (SA) → typically produces Weber A fractures
- Supination-External Rotation (SER) → the most common pattern, typically produces Weber B fractures
- Pronation-Abduction (PA) → typically produces Weber B or C fractures
- Pronation-External Rotation (PER) → typically produces Weber C fractures, often at a high level
Understanding the Lauge-Hansen mechanism helps surgeons anticipate which ligaments are likely injured even before stress testing, making it a useful companion to the Weber system in complex cases.
Weber Classification Radiology Guide
Radiological evaluation is crucial for proper classification.
How to Identify Weber Type on X-ray
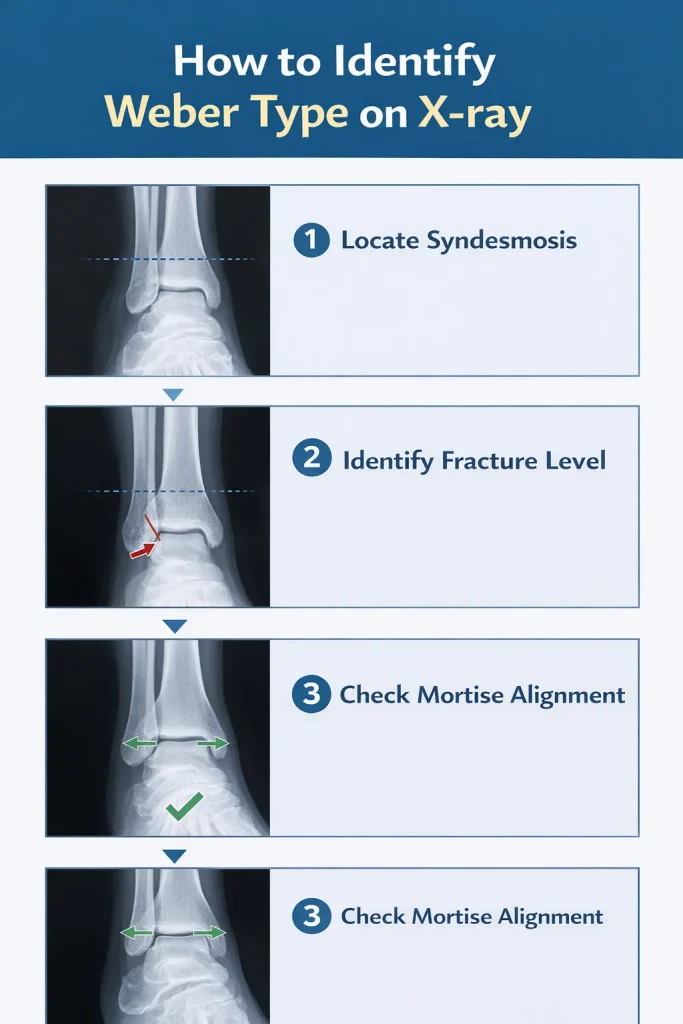
Steps:
- Identify the fibular fracture location
- Assess relationship to syndesmosis
- Check the medial clear space
- Look for talar shift
Importance of Mortise View

The mortise view allows:
- Assessment of joint alignment
- Evaluation of medial clear space
- Detection of syndesmotic widening
Radiology plays a central role in determining stability and the need for surgery.
Key Radiological Measurements
Knowing specific radiological measurements helps in precise classification and surgical decision-making:
- Medial clear space: Normal is ≤4 mm. Values above this suggest deltoid ligament disruption or talar shift.
- Tibiofibular clear space: Should be <6 mm on AP view. Widening suggests syndesmotic disruption.
- Tibiofibular overlap: Should be ≥6 mm on AP view and ≥1 mm on mortise view. Reduced overlap suggests syndesmotic widening.
- Talocrural angle: Normally 8-15 degrees. Significant asymmetry compared to the opposite ankle is clinically significant.
These measurements are particularly important in Weber B fractures where stability is uncertain, and treatment decisions depend on subtle radiological findings.
Weber Classification Radiology: CT Scan Role
While plain X-rays are used for initial classification, CT scanning plays an important role in complex fractures:
- Identifies associated posterior malleolus fractures
- Assesses the size of the posterior malleolus fragment
- Evaluates articular surface involvement
- Guides surgical planning for comminuted fractures
- Identifies subtle syndesmotic widening not seen on plain films
In Weber C fractures, especially, CT is recommended to ensure no posterior malleolus fragment is missed before surgical planning.
Radiology plays a central role in determining stability and the need for surgery.
Treatment Based on Weber Type
Treatment decisions depend on stability.
- Weber A → Conservative treatment
- Weber B → Conservative or surgical
- Weber C → Usually surgical
Surgical options include:
- Open reduction and internal fixation (ORIF)
- Syndesmotic screw fixation
- Plate fixation
Dr Divya Ahuja specializes in managing complex ankle fractures with emphasis on anatomical restoration and functional recovery.
Weber Classification and Management: Decision Framework
Choosing the right treatment for each Weber type requires a structured assessment. Here is how orthopedic surgeons approach management decisions:
Weber A Management
- Confirm fracture is isolated and below the syndesmosis
- No stress testing required in most cases
- Begin weight-bearing as tolerated in a boot or short-leg cast
- Follow up at 6 weeks with a repeat X-ray
- Physiotherapy once the fracture unites
Weber B Management
- Perform a mortise view X-ray
- Measure medial clear space
- If borderline: perform stress X-ray (gravity or manual external rotation)
- Stable → Boot or cast, partial weight-bearing, serial radiographs
- Unstable → ORIF fibula ± syndesmotic fixation ± medial-side repair
- Follow up at 2, 6, and 12 weeks
Weber C Management
- Assume syndesmotic instability until proven otherwise
- CT scan to assess posterior malleolus
- Plan ORIF fibula with plate
- Test the syndesmosis intraoperatively under fluoroscopy
- Proceed with syndesmotic fixation (screw or suture button)
- Non-weight-bearing for 6-8 weeks post-surgery
- Physiotherapy at 8-12 weeks, depending on fixation
This structured approach ensures no injury component is missed, which is the most common cause of poor outcomes after ankle fractures.
Recovery Based on Weber Type
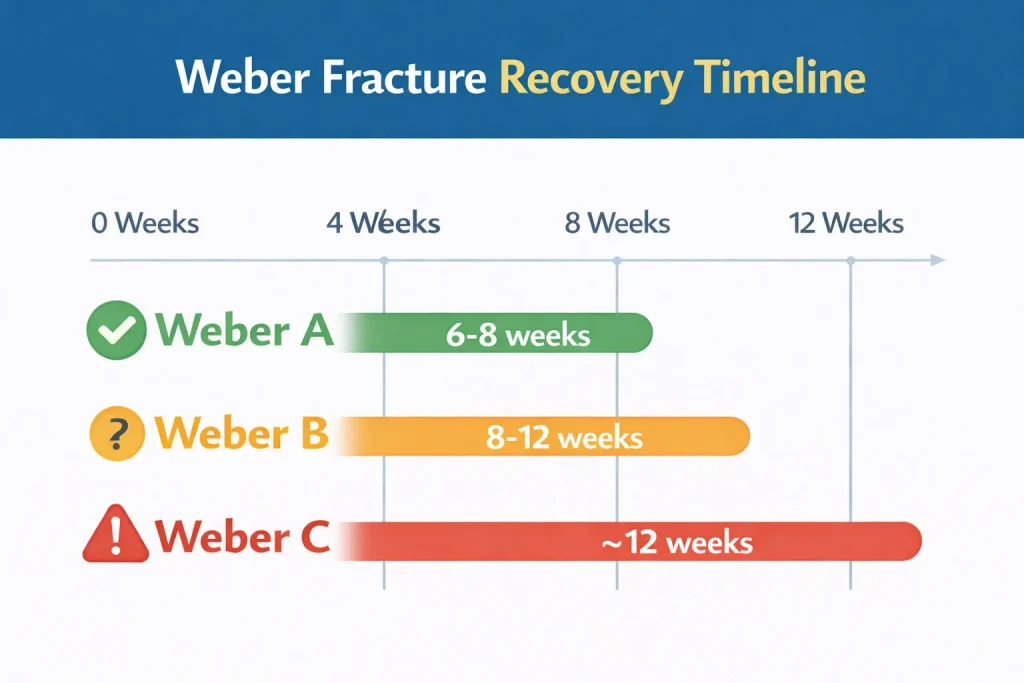
Healing times vary depending on severity.
| Type | Healing Time | Surgery Required |
|---|---|---|
| Weber A | 6–8 weeks | Rare |
| Weber B | 8–12 weeks | Sometimes |
| Weber C | 3–6 months | Common |
Rehabilitation includes:
- Range of motion exercises
- Strengthening
- Balance training
- Gradual return to activity
Swelling may persist for several months.
Weber C Fracture Recovery Time: What to Expect
Weber C fracture recovery is the longest and most involved of the three types. Here is a realistic timeline for patients:
Weeks 1-2: Post-operative pain management, limb elevation, wound care. Non-weight-bearing on crutches.
Weeks 2-6: Continued non-weight-bearing. Gentle range of motion exercises of the toes and knee to prevent stiffness. The syndesmotic screw is typically retained during this phase.
Weeks 6-8: Begin partial weight-bearing if fracture healing is confirmed on X-ray. Syndesmotic screw removal may be planned at this stage (if a metallic screw was used rather than a suture button).
Weeks 8-12: Transition to full weight-bearing. Active physiotherapy begins – focusing on ankle range of motion, calf strengthening, and proprioception.
3-6 months: Most patients achieve functional walking. Return to sport or physically demanding work typically occurs at 4-6 months, depending on fixation type and individual healing.
Important: Even after fracture healing, soft tissue healing around the syndesmosis takes longer. Patients should expect residual swelling and stiffness for 6-12 months after a Weber C injury. This is normal and not a sign of failure.
Complications
Potential complications include:
- Chronic ankle instability
- Post-traumatic arthritis
- Malunion
- Nonunion
- Syndesmotic failure
Early diagnosis and appropriate treatment reduce long-term risks.
When to See an Orthopedic Specialist
Seek medical attention if:
- Severe ankle pain
- Swelling
- Inability to bear weight
- Deformity
- Injury after twisting or falling
Early intervention improves outcomes.
Treatment in India & International Consultation
Many global patients seek ankle fracture treatment in India due to high-quality care and affordability.
Dr Divya Ahuja provides advanced treatment for Weber fractures, including:
- Precise fracture fixation
- Syndesmotic stabilization
- Comprehensive rehabilitation
International patients benefit from:
- Online consultations
- Treatment planning
- Affordable surgical care
- Postoperative support
Conclusion
The Weber classification remains one of the most practical systems for categorizing ankle fractures. Assessing the level of fibular fracture relative to the syndesmosis helps determine stability, treatment approach, and recovery expectations. With timely diagnosis and appropriate management, most patients achieve good functional recovery and return to normal activities.
Explore all our fracture-related blogs
| Topic | Link |
| Cervical Radiculopathy | Click here |
| Distal Radius Fracture | Click here |
| Proximal Humerus Fracture | Click here |
| Lauge-Hansen Classification of Ankle Fractures | Click here |
| Weber Classification of Ankle Fractures | Click here |
| Trimalleolar Fracture | Click here |
| Bimalleolar Ankle Fracture | Click here |
| Lateral Malleolus Fracture | Click here |
| Medial Malleolus Fracture | Click here |
| Complete Guide to Ankle Fractures | Click here |
| Femur Shaft Fractures | Click here |
| Tibia Fracture | Click here |
FAQs
What is Weber’s classification of ankle fractures?
Weber classification is a system used to categorize ankle fractures based on the level of fibular fracture relative to the syndesmosis. It divides fractures into Weber A, B, and C types, helping determine ankle stability and whether surgery is required.
What is a Weber B fracture, and does it need surgery?
A Weber B fracture occurs at the level of the syndesmosis and is the most common ankle fracture type. Surgery is required only if there is ankle instability, talar shift, or ligament injury; stable Weber B fractures can often heal with a cast or boot.
How long does a Weber B fracture take to heal?
A stable Weber B fracture usually heals within 6–8 weeks, but full recovery, including strength and mobility, may take 3–4 months. Surgical cases may require longer rehabilitation depending on fixation and syndesmotic involvement.
What is the difference between Weber B and Weber C fractures?
The main difference is fracture level. Weber B occurs at the syndesmosis level and may be stable or unstable, while Weber C occurs above the syndesmosis and is usually unstable, often requiring surgical fixation and syndesmotic stabilization.
Is Weber A fracture considered stable?
Yes, Weber A fractures occur below the syndesmosis and are generally stable because the ligament complex remains intact. Most Weber A fractures can be treated conservatively with immobilization and gradual weight-bearing.
What are the radiology findings in the Weber classification?
Radiology findings include identifying the fibular fracture level on X-ray relative to the syndesmosis. Mortise view helps assess medial clear space, talar shift, and syndesmotic widening, which determine fracture stability and need for surgery.
Can a Weber fracture heal without surgery?
Many Weber A and some Weber B fractures can heal without surgery if the ankle joint remains stable and aligned. However, Weber C fractures and unstable Weber B fractures typically require surgical fixation for proper healing.
Which Weber fracture type is most serious?
Weber C fractures are generally the most serious because they occur above the syndesmosis and often involve ligament disruption, leading to ankle instability that usually requires surgical fixation.
What is a syndesmotic injury in Weber fractures?
A syndesmotic injury occurs when the ligaments connecting the tibia and fibula are damaged. It is commonly associated with Weber B and Weber C fractures and may require syndesmotic screw or tightrope fixation to restore stability.
How do doctors identify the Weber classification on ankle X-ray?
Doctors identify Weber type by locating the fibular fracture and comparing its level to the syndesmosis on X-ray. Mortise view helps assess joint alignment and detect instability, which guides treatment planning.
What is the difference between a stable and unstable Weber B fracture?
A stable Weber B fracture has an intact syndesmosis and no talar shift, making conservative treatment with a cast or boot appropriate. An unstable Weber B fracture involves disruption of the syndesmosis or deltoid ligament, causing talar shift and requiring surgical fixation to restore ankle alignment.
How long does Weber C fracture recovery take?
Weber C fracture recovery typically takes 3-6 months for functional recovery. Patients remain non-weight-bearing for 6-8 weeks after surgery, begin physiotherapy at 8-12 weeks, and return to normal activities between 4-6 months. Residual swelling and stiffness can persist for up to 12 months.
What is the Danis-Weber classification?
The Danis-Weber classification is the full name of the Weber classification system. It was originally described by Robert Danis in 1949 and later refined by Bernhard Georg Weber in 1966. The three-type system (A, B, C) is based on the level of the fibular fracture relative to the syndesmosis and remains the gold standard for ankle fracture classification.
Is Weber C fracture conservative treatment ever appropriate?
Weber C fractures are almost always treated surgically because the syndesmosis is disrupted. Conservative treatment is only considered in rare situations – such as elderly or medically unfit patients – and carries a higher risk of malunion and ankle arthritis. Any decision to manage a Weber C fracture conservatively should be made by an experienced orthopedic specialist.