Shoulder pain often begins quietly. A slight discomfort when you lift your arm, a dull ache after the gym, or stiffness that shows up each morning and slowly fades. Most people ignore it at first, expecting it to pass on its own. But when that pain keeps returning – especially during simple movements like reaching overhead or putting on a shirt – it is rarely just muscle fatigue. It is usually your body signaling something specific: shoulder impingement or rotator cuff tendinitis.
These are not problems limited to athletes or manual workers. Today, they are among the most common musculoskeletal conditions seen across all age groups. People with desk jobs, long screen hours, poor posture habits, and inconsistent physical activity are developing shoulder problems at increasing rates. The shoulder is the most mobile joint in the body, and that mobility comes at the cost of stability. When the balance between movement and support breaks down, pain follows.
This guide gives you a complete, practical understanding of Shoulder Impingement and Rotator Cuff Tendinitis – what is actually happening inside the joint, why the pain appears when you lift your arm, how to identify early symptoms, and how to treat and prevent it effectively on your own.
Table of Contents
What is Shoulder Impingement?
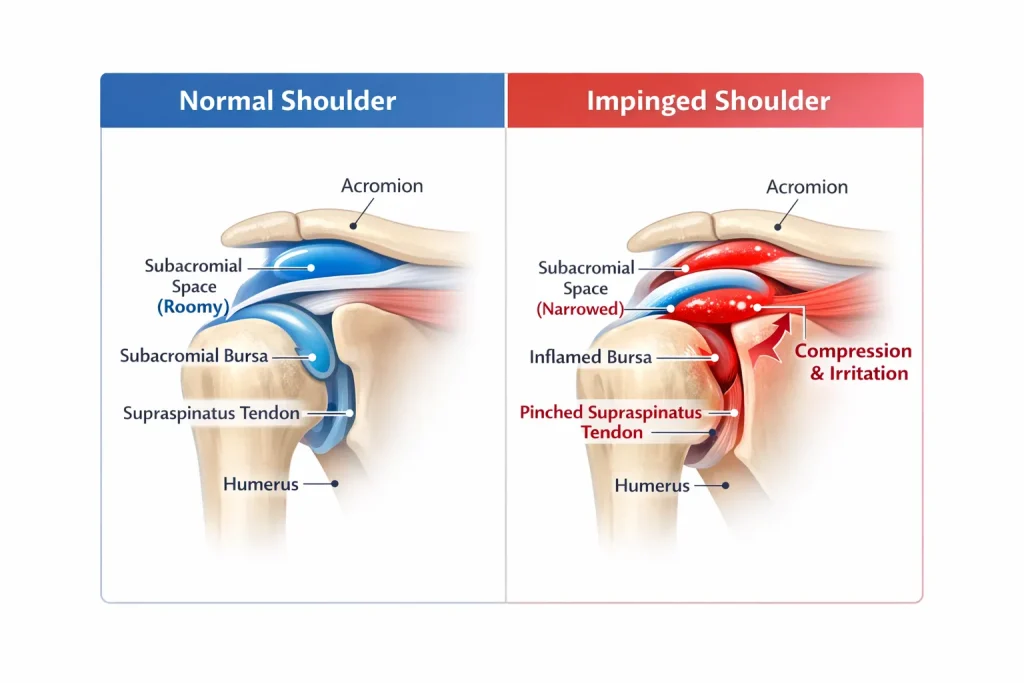
Shoulder impingement is a condition where the soft tissues inside the shoulder – primarily the rotator cuff tendons – get mechanically compressed between the bones during arm movement. This compression happens in the subacromial space, a narrow gap between the head of the upper arm bone and the acromion, which is the bony roof formed by the outer part of the shoulder blade.
When you raise your arm, this space naturally becomes smaller. If it is already reduced due to inflammation, poor posture, or structural changes in the joint, the tendons and the bursa sac get pinched with every movement. This repeated pinching is what defines shoulder impingement syndrome.
Over time, the tendons respond to that repeated friction by becoming inflamed and irritated. This is when the problem progresses into rotator cuff tendinitis – active inflammation of the tendon tissue. If the irritation continues without treatment, the tendon structure begins to break down. At that stage, it becomes rotator cuff tendinopathy or tendinosis, both of which describe chronic, degenerative changes that take significantly longer to recover from.
Understanding this progression matters because it explains why early treatment always produces faster and more complete results than waiting until the pain becomes severe.
What happens mechanically during shoulder impingement:
- The subacromial space narrows as the arm is elevated
- The rotator cuff tendon gets pinched between the acromion and the upper arm bone
- The bursa sac between these structures also gets compressed and inflamed
- Repeated pinching causes swelling, friction, and gradual tendon damage over time
Shoulder Anatomy and Why It Makes Impingement Common
The shoulder joint is built for maximum range of motion. It is a ball-and-socket structure where the rounded head of the humerus sits in a shallow cup on the shoulder blade, called the glenoid. Four muscles and their tendons form the rotator cuff, wrapping around this joint to stabilize and move the arm.
The most important of these for understanding impingement is the supraspinatus muscle. It runs along the top of the shoulder blade, and its tendon passes directly through the subacromial space on its way to the upper arm bone. Because of this location, the supraspinatus is the first tendon to get compressed when that space narrows. Supraspinatus tendinitis and supraspinatus impingement are therefore the most common diagnoses in this condition.
Sitting between the rotator cuff tendon and the underside of the acromion is the subacromial bursa – a small fluid-filled sac whose job is to reduce friction during arm movement. When impingement occurs repeatedly, this bursa becomes inflamed alongside the tendons, a condition called subacromial bursitis.
The shape of the acromion itself also plays a role. A flat acromion provides more space. A curved or hooked acromion – known as a type II acromion – naturally reduces the subacromial space, making impingement significantly more likely regardless of posture or muscle strength. Bone spurs forming on the underside of the acromion over time can further narrow this space.
Key structures involved in shoulder impingement:
- Supraspinatus tendon – most frequently compressed
- Subacromial bursa – becomes inflamed alongside the tendon
- Acromion shape – determines how much space is naturally available
- Shoulder blade (scapula) – its movement directly affects joint mechanics
- Glenohumeral joint ligaments – contribute to overall shoulder stability
Why Does Shoulder Pain Occur When Lifting Your Arm
The most frustrating feature of shoulder impingement is the way pain appears during certain movements but not others. This confuses many people and leads them to delay seeking an explanation. The pain is not random – it follows a very predictable mechanical pattern.
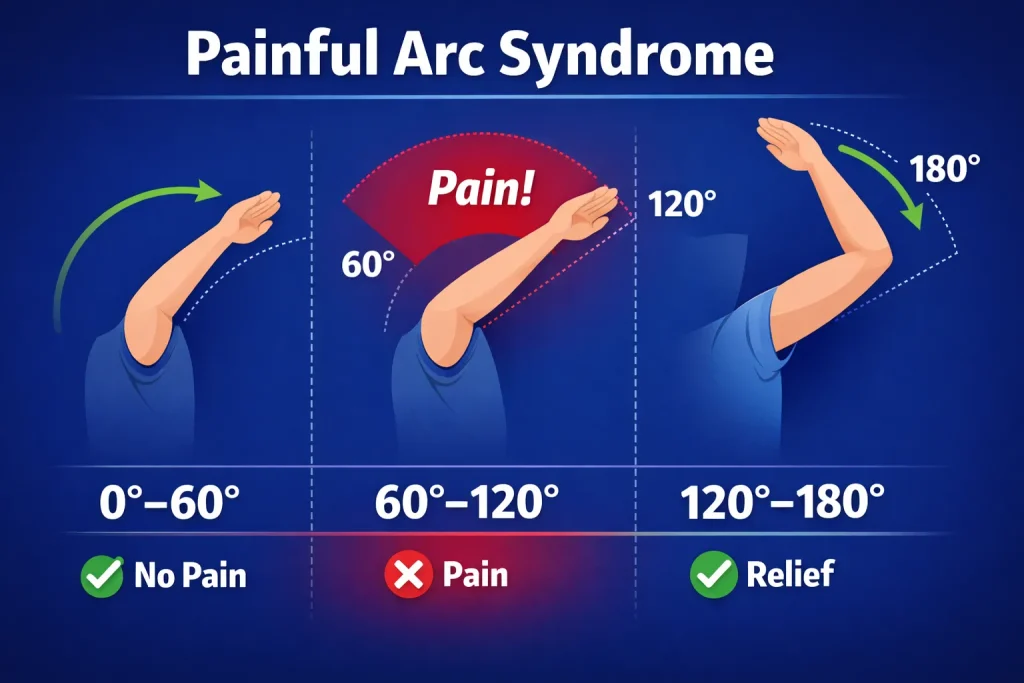
When you elevate your arm, the subacromial space shrinks at a specific point in the movement range. If the rotator cuff tendon is already thickened or inflamed, it gets pinched between the acromion and the humeral head during this part of the movement. This produces the characteristic pattern known as painful arc syndrome.
The painful arc in shoulder impingement typically appears between 60 and 120 degrees of arm elevation. Below 60 degrees, there is usually no pain because the tendon is not yet being compressed. Between 60 and 120 degrees, the pinching occurs and pain spikes. Above 120 degrees, the mechanics of the joint shift and the compression eases – so many people find the pain actually reduces again at full overhead elevation.
This is why shoulder pain when lifting your arm halfway is so specific to impingement. Everyday actions like reaching for something on a high shelf, pulling on a shirt, combing your hair, or reaching across the body suddenly trigger that familiar pain while other movements feel relatively normal.
Shoulder pain radiating down the arm is also common, particularly along the outer upper arm toward the elbow. This happens because the inflamed tendons and bursa refer pain into the deltoid muscle distribution. If pain travels all the way to the hand with numbness or tingling, that pattern suggests nerve involvement – either a pinched nerve in the shoulder or a problem in the cervical spine – rather than simple impingement.
Symptoms of Rotator Cuff Tendinitis and Shoulder Impingement

Rotator cuff tendinitis symptoms develop gradually over weeks or months. Many people dismiss early warning signs as temporary strain and only start taking the condition seriously once it is well established. Catching symptoms early cuts recovery time significantly.
Symptoms to recognize:
- Shoulder pain when lifting the arm to the side or forward
- Front shoulder pain or pain on the top of the shoulder
- Pain appearing in the 60 to 120 degree arc of arm elevation
- Shoulder pain radiating down the arm toward the elbow
- Night-time shoulder pain, especially when lying on the affected shoulder
- Shoulder stiffness in the morning that gradually loosens with movement
- Weakness when rotating, lifting, or reaching with the affected arm
- A dull, burning sensation deep inside the shoulder joint
- Pain that worsens during overhead activities or shoulder pain while working out
- Shoulder pain and swelling in some cases, particularly with concurrent bursitis
Left shoulder pain vs right shoulder pain – both sides are equally susceptible to impingement. The affected side usually reflects your dominant arm, your sport, or the physical demands of your work. Left side shoulder pain that also involves chest tightness, jaw discomfort, or breathlessness must always be assessed medically first before assuming it is mechanical in origin.
Bilateral shoulder pain – pain in both shoulders at the same time – is less common with pure impingement and may suggest a systemic cause such as inflammatory arthritis or spondylitis. Shoulder pain spondylitis – where cervical or thoracic spine degeneration contributes to shoulder symptoms – is an important consideration in people with concurrent neck pain and shoulder pain on the left or right side.
What Causes Shoulder Impingement
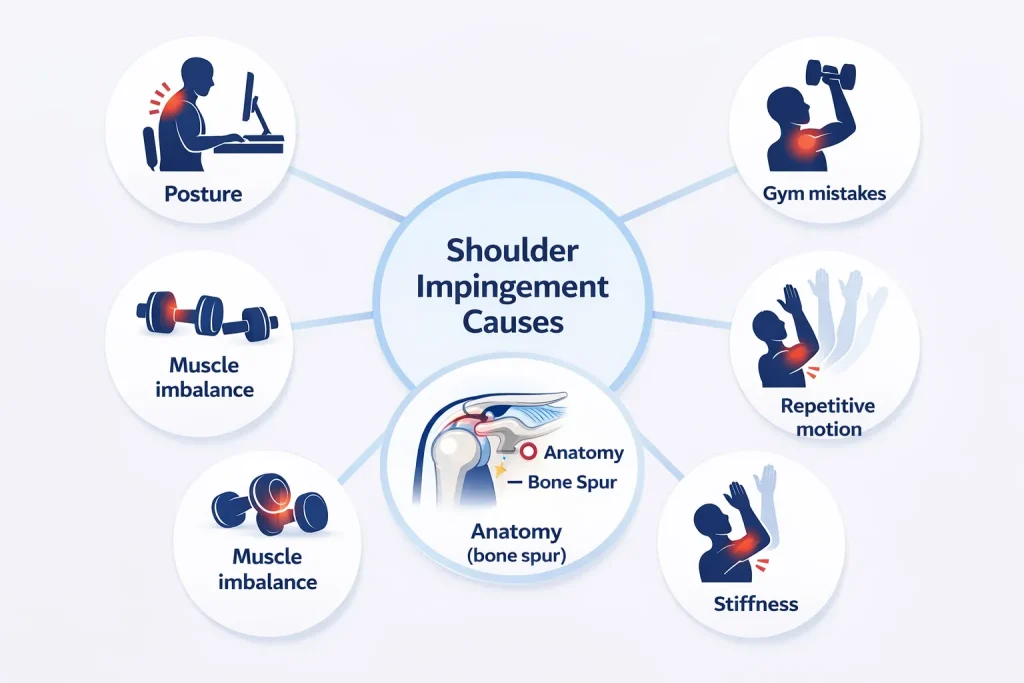
Shoulder impingement builds gradually through a combination of mechanical, postural, and lifestyle factors. It is rarely the result of a single incident. Identifying your specific cause is critical because without addressing it, symptoms will keep returning no matter how well you treat the pain itself.
Postural and movement-related causes:
- Rounded shoulders and forward head posture from prolonged desk work, phone use, or driving
- Repetitive overhead movement in sport or work – swimming, throwing, painting, plastering, tennis
- Poor technique during gym exercises, particularly overhead press, lateral raises, and bench press
- Sleeping in positions that hold the shoulder in prolonged internal rotation throughout the night
Muscle-related causes:
- Weak rotator cuff muscles that fail to properly center the arm in the shoulder socket during movement
- Tight chest muscles and overactive front deltoid pulling the shoulder into a rounded, internally rotated position
- Weak rear deltoid and posterior shoulder muscles creating an imbalance in shoulder mechanics
- Poor scapular control caused by weak lower trapezius and serratus anterior muscles
- Deltoid tendonitis or pulled deltoid from overtraining without adequate rotator cuff support
Structural causes:
- Type II acromion shape naturally reducing subacromial space
- Bone spurs forming on the underside of the acromion over years of friction
- Age-related rotator cuff degeneration – tendon tissue loses water content, strength, and elasticity over time
- Calcific tendinitis of the shoulder – calcium deposits forming within the tendon, causing acute severe pain episodes
- Previous shoulder muscle injury or pulled shoulder muscle that healed with reduced strength and altered mechanics
How to Identify Shoulder Impingement Yourself
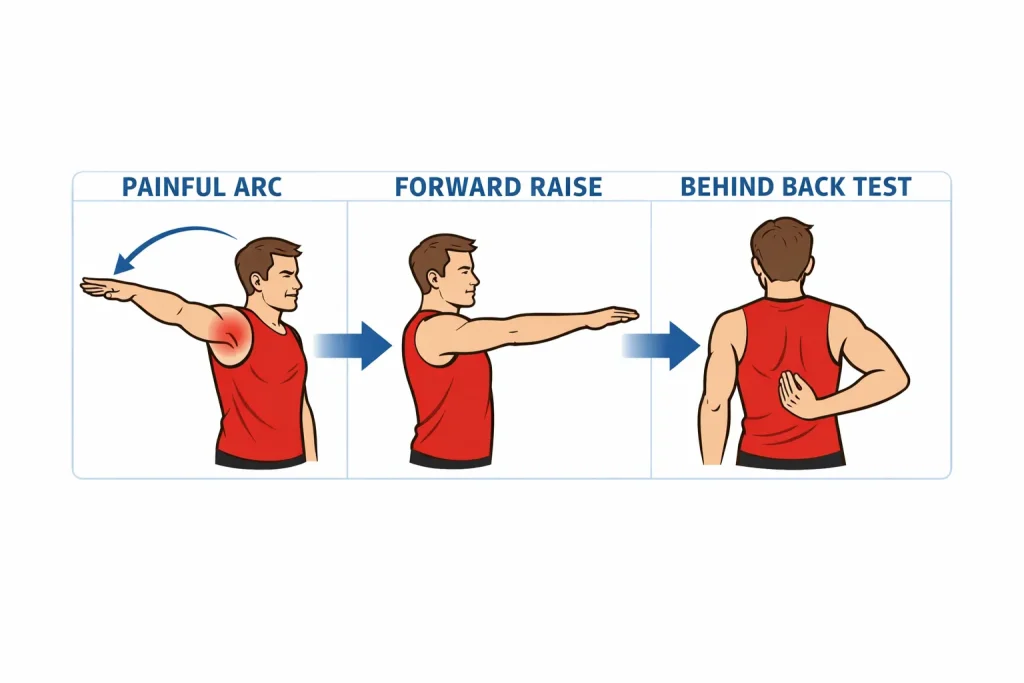
Three simple tests done at home can help you determine whether your shoulder pain pattern is consistent with impingement before beginning self-treatment.
Painful arc test: Slowly raise your arm out to the side from your body. Note exactly where pain begins and ends. Pain that appears between 60 and 120 degrees of elevation and then reduces above that range is the defining sign of shoulder impingement syndrome.
Forward elevation test: With your arm straight and palm facing downward, raise it forward as high as you comfortably can. Reproduction of your usual front shoulder pain or shoulder tip pain during this movement strongly implicates the supraspinatus tendon.
Internal rotation assessment: Reach your affected arm behind your lower back and note how far up your spine you can comfortably reach. Compare it to the unaffected side. Significant restriction indicates posterior shoulder tightness and shoulder internal rotation pain – both consistent with established impingement.
Complete DIY Treatment Plan for Shoulder Impingement
The most important thing to understand about treating shoulder impingement yourself is that it requires a structured, progressive approach. Doing random stretches occasionally or simply resting will not produce lasting relief. The four-phase plan below addresses pain first, then mobility, then strength, then return to full activity – in that order.
Phase One: Reduce Pain and Calm the Tissues (Week 1 to 2)
The immediate goal is settling the inflamed tendons and bursa. This means relative rest – not complete immobilization, but removing the specific movements that trigger your pain while keeping the shoulder gently active.
What to do:
- Apply ice wrapped in a cloth to the front and side of the shoulder for 15 to 20 minutes, two to three times daily during the first week
- Stop all overhead reaching, behind-the-back movements, and sleeping on the affected shoulder
- Use anti-inflammatory shoulder pain medicine if suitable for your health – ibuprofen taken consistently for a short period reduces tendon inflammation more effectively than single doses
- Adjust your sitting posture immediately – screen at eye level, shoulders relaxed and back, feet flat on the floor
- Temporarily stop gym exercises that reproduce shoulder pain, including overhead press and lateral raises
Phase Two: Restore Shoulder Movement (Week 2 to 4)
Once acute pain settles, begin gentle mobility work to restore the normal range of motion. The goal at this stage is movement – not strength, not stretching to the point of pain.
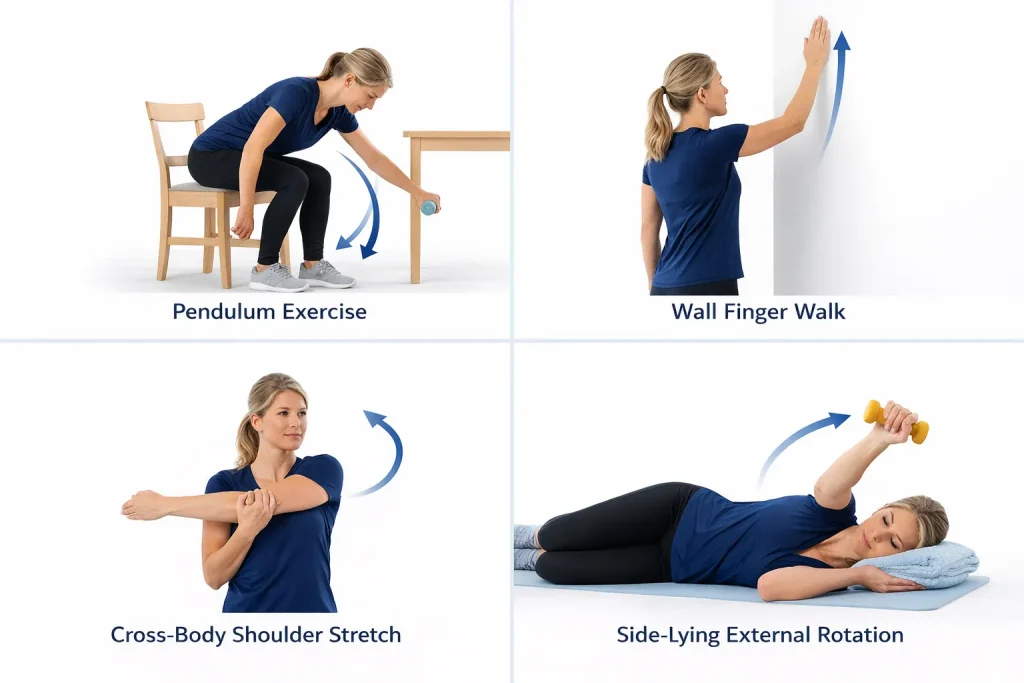
Exercises for this phase:
- Pendulum exercise: Lean forward over a table, let the affected arm hang freely, and make small, gentle clockwise and counterclockwise circles using gravity rather than muscle effort. One to two minutes, twice daily
- Wall finger walk: Face a wall and slowly walk your fingers upward as high as comfort allows. Hold for five seconds, then walk back down. Ten repetitions
- Cross-body stretch: Pull the affected arm across your chest using the opposite hand. Hold 30 seconds, three times. This targets posterior shoulder tightness – the most consistent finding in shoulder impingement
- Sleeper stretch: Lie on the affected side with your arm at 90 degrees in front. Gently push your forearm downward with the other hand. Hold 30 seconds. Three sets. This addresses the posterior capsule tightness that directly contributes to subacromial impingement
Phase Three: Strengthen the Rotator Cuff (Week 4 to 8)
This is the most important phase and the one most commonly skipped. Rotator cuff strengthening is what stops the shoulder from re-impinging. Without this work, pain returns – often within weeks of feeling better.
Strengthening exercises:
- External rotation with resistance band: Stand with your elbow fixed at your side, bent at 90 degrees. Hold a light resistance band and rotate your forearm outward, away from your body. Return slowly. Three sets of 15 repetitions. This directly targets the lateral rotation of the shoulder joint muscles
- Side-lying external rotation: Lie on the unaffected side with a light dumbbell. Rotate your forearm upward like slowly opening a book. Lower under control. Three sets of 12 repetitions
- Scapular retraction: Sitting or standing, draw your shoulder blades gently back and downward – away from your ears, toward the opposite back pocket. Hold for five seconds. Fifteen repetitions. This single exercise improves shoulder blade positioning and directly increases the subacromial space during arm movements
- Prone Y exercise: Face down on a bed edge with the affected arm hanging. Raise the arm into a Y shape with the thumb pointing upward. Lower slowly. Three sets of 10. This targets the lower trapezius, which is consistently weak in people with shoulder impingement syndrome
Critical habit to build: Before every exercise, and before any overhead movement during recovery, consciously set your shoulder blade – draw it gently back and downward. This posture reset mechanically opens the subacromial space and protects the tendon from compression during movement. Practice it until it becomes completely automatic.
Phase Four: Return to Full Activity (Week 8 to 12)
As shoulder pain resolves and strength rebuilds, gradually reintroduce heavier activities and overhead work. The most common cause of relapse is returning to full activity too soon.
Return-to-activity guidelines:
- Complete at least eight weeks of pain-free rotator cuff strengthening before returning to overhead pressing at the gym
- When returning, reduce weights significantly and prioritize technique over load
- Perform band warm-up exercises before every upper-body training session as a permanent habit
- If shoulder pain after gym sessions returns, reduce load immediately and return to phase three for two more weeks before progressing again
- Keep external rotation and scapular exercises as a regular maintenance routine, even when fully recovered
How to Sleep With Shoulder Impingement Pain
Night-time shoulder pain is one of the most disruptive features of rotator cuff tendinitis. Lying on the impinged shoulder compresses the subacromial space continuously through the night, disrupting sleep and slowing recovery.
Best positions for sleeping:
- On your back with a small pillow under the affected arm – this keeps the shoulder in a slightly elevated, neutral position that reduces subacromial compression
- On your unaffected side, while hugging a pillow to your chest, this prevents the sore arm from rolling forward into internal rotation
- Never on the impinged shoulder directly
- Avoid tucking the affected arm under the pillow – this forces sustained shoulder internal rotation and significantly worsens overnight tendon irritation
Shoulder Impingement Recovery Time: What to Realistically Expect
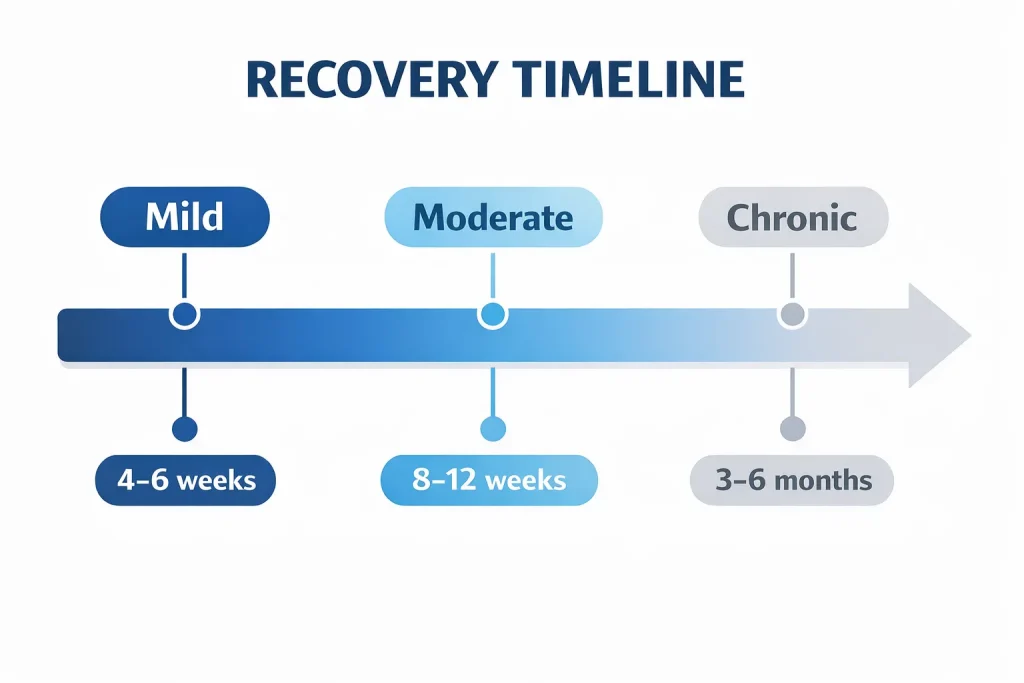
Recovery timelines depend on how long the condition has been developing and how consistently the treatment plan is followed.
- Mild shoulder impingement caught early: 4 to 6 weeks with consistent self-care
- Moderate rotator cuff tendinitis: 8 to 12 weeks
- Chronic rotator cuff tendinopathy or tendinosis: 3 to 6 months
- Calcific tendinitis of the shoulder: variable, may require medical evaluation if not improving with conservative care
- Shoulder impingement with concurrent subacromial bursitis: slightly longer due to dual-structure involvement
The most important predictor of recovery speed is not the severity of the initial pain – it is how consistently the phase three strengthening exercises are performed. People who follow a structured rotator cuff programme recover faster and relapse far less often than those relying solely on rest or passive pain relief.
Read: Complete Guide to Shoulder Exercises for Strength, Mobility, and Rotator Cuff Rehabilitation
When to See a Doctor
Self-directed treatment is appropriate and effective for most cases of shoulder impingement and rotator cuff tendinitis. However, some presentations require professional evaluation.
See a doctor or shoulder pain doctor if:
- Shoulder pain followed a direct fall, collision, or impact
- Sudden severe pain occurs with significant arm weakness – possible rotator cuff tear
- Shoulder pain radiating to the hand with numbness or tingling – possible pinched nerve in the shoulder or cervical spine problem
- Left shoulder pain accompanies chest tightness or jaw discomfort
- Swelling on shoulder near neck or visible deformity is present
- Pain is not improving after eight weeks of consistent home rehabilitation
- You have been told you have a type II acromion or calcific tendinitis that is not responding to conservative treatment
Prevention: Keeping Your Shoulders Healthy Long Term
Prevention is far less demanding than treatment. A few consistent habits protect the shoulder joint from the mechanical stress that leads to impingement.
Long-term prevention habits:
- Strengthen the rotator cuff and rear deltoid muscles regularly as a permanent part of your fitness routine
- Maintain correct posture at your desk – screen at eye level, shoulders relaxed, upper back gently supported
- Avoid prolonged overhead work without regular breaks to lower and rest the arms
- Stretch the chest and front shoulder muscles daily to counteract the shortening caused by desk work and forward-head posture
- Warm up the rotator cuff with band exercises before any upper-body training session
- Take regular movement breaks during long periods of sitting – even standing and rolling your shoulders briefly every 45 minutes makes a measurable difference over time
Conclusion
Shoulder impingement and rotator cuff tendinitis are painful, progressive, and entirely manageable – when you understand what is driving them and approach recovery with a clear plan.
The pain you feel when lifting your arm is not arbitrary. It is a direct mechanical signal from a specific structure under compression. By learning to read that signal, addressing the root causes of muscle imbalance and poor posture, and following a structured four-phase rehabilitation plan, most people achieve a full recovery without needing clinic visits, injections, or surgery.
The key is not just treating symptoms – it is removing what caused the impingement in the first place, rebuilding the rotator cuff strength that prevents recurrence, and maintaining those habits long after the pain has gone. Be consistent, respect the recovery timeline, and keep the shoulder strong permanently. That is the difference between a temporary fix and a lasting solution.
Frequently Asked Questions
What is shoulder impingement?
Shoulder impingement is a condition where the rotator cuff tendons get compressed in the subacromial space during arm movement. Repeated compression causes inflammation and pain, particularly when lifting the arm.
Why does my shoulder hurt when I lift my arm?
Pain occurs because the inflamed tendon gets pinched between the acromion and the upper arm bone during a specific range of elevation. This produces the characteristic painful arc between 60 and 120 degrees.
Can shoulder impingement heal without surgery?
Yes. The vast majority of cases respond well to rest, targeted rotator cuff strengthening, posture correction, and activity modification. Surgery is rarely needed and only considered after thorough conservative treatment has failed.
How long does rotator cuff tendinitis take to heal?
Mild cases improve in 4 to 6 weeks. Moderate tendinitis takes 8 to 12 weeks. Chronic tendinopathy can take 3 to 6 months, particularly if it has been building for a long time without proper rehabilitation.
What is the fastest way to relieve shoulder pain at home?
Rest the shoulder from provocative movements, apply ice consistently to reduce inflammation, correct your sitting posture, and begin gentle mobility work as soon as pain allows. Starting rotator cuff strengthening exercises as early as appropriate is the most important step for lasting relief.
When should I see a doctor for shoulder pain?
Seek medical attention if pain follows an injury, if you experience sudden weakness suggesting a tear, if numbness or tingling radiates into the hand, or if pain is not improving after 8 weeks of consistent self-directed rehabilitation.