You reach up to grab something from a high shelf – and your shoulder says no. The pain can be dull and nagging or sharp and sudden. Either way, it stops you from doing everyday things: combing your hair, reaching across a table, or sleeping through the night.
For millions of people worldwide, that pain has a name: a rotator cuff tear.
Nearly 2 million people visit their doctor every year because of rotator cuff injuries. Many more never go, assuming the pain is just stiffness or a pulled shoulder muscle that will heal on its own.
Sometimes it does. Often, it does not – and waiting too long can turn a manageable shoulder muscle tear into a problem that requires surgery.
This guide gives you a complete, honest picture of what a rotator cuff injury is, why it happens, what symptoms to watch for, and what your real treatment options look like. Whether you have just been diagnosed, are managing long-standing rotator cuff pain, or simply want to understand the shoulder structure better, this article is your starting point.
Table of Contents
What is a Rotator Cuff? Anatomy You Need to Know
Before understanding a rotator cuff tear, it helps to understand what the rotator cuff actually is and what it does.
The shoulder is a ball-and-socket joint. The ball is the head of your humerus (upper arm bone), and the socket is a shallow cup in your scapula (shoulder blade). The clavicle (collarbone) completes the trio of bones that form the joint.
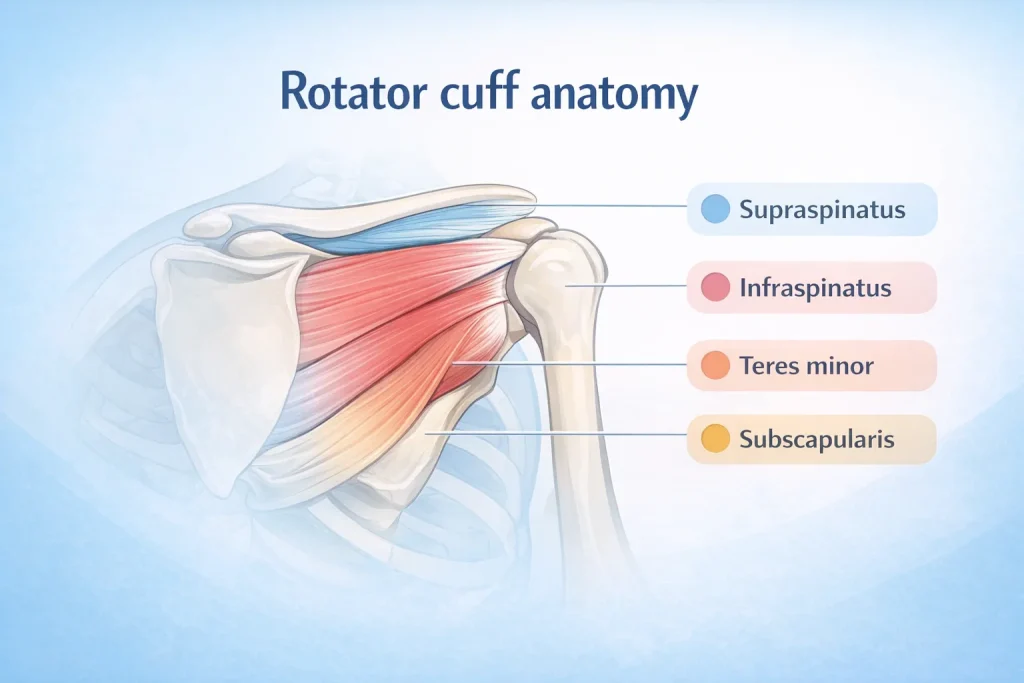
The rotator cuff is a group of four muscles and their tendons that wrap around the ball, keeping the arm seated firmly in the socket while also powering the lifting and rotating movements you make constantly throughout the day. When orthopaedic specialists talk about the shoulder cuff, this is exactly what they mean.
The Four Rotator Cuff Muscles – SITS
Orthopaedic specialists use the acronym SITS to remember the four rotator cuff muscles:
- Supraspinatus – runs along the top of the shoulder blade and lifts the arm sideways. This is the most commonly torn muscle in a rotator cuff injury. The supraspinatus tendon is also the area most frequently highlighted in any rotator cuff diagram.
- Infraspinatus – located at the back of the shoulder blade; rotates the arm outward. An infraspinatus tear is the second most common type of rotator cuff injury.
- Teres Minor – works alongside the infraspinatus to assist outward rotation of the arm.
- Subscapularis – sits on the front of the shoulder blade and rotates the arm inward. It forms the front portion of the musculotendinous cuff of the shoulder.
Together, these four muscles and their tendons form a strong, dynamic cuff around the head of the humerus. The rotator cuff muscles function as both stabilisers and movers – every time you raise, rotate, or lower your arm, all four are working together.
The Role of the Bursa
Between the rotator cuff tendons and the bone above the shoulder (the acromion) sits a small lubricating sac called the bursa. In a healthy shoulder, the bursa allows the rotator cuff tendons to glide freely when you move your arm. When a rotator cuff injury occurs, this bursa often becomes inflamed too, producing the additional burning, swelling, and pain that makes the condition feel worse.
Types of Rotator Cuff Tears
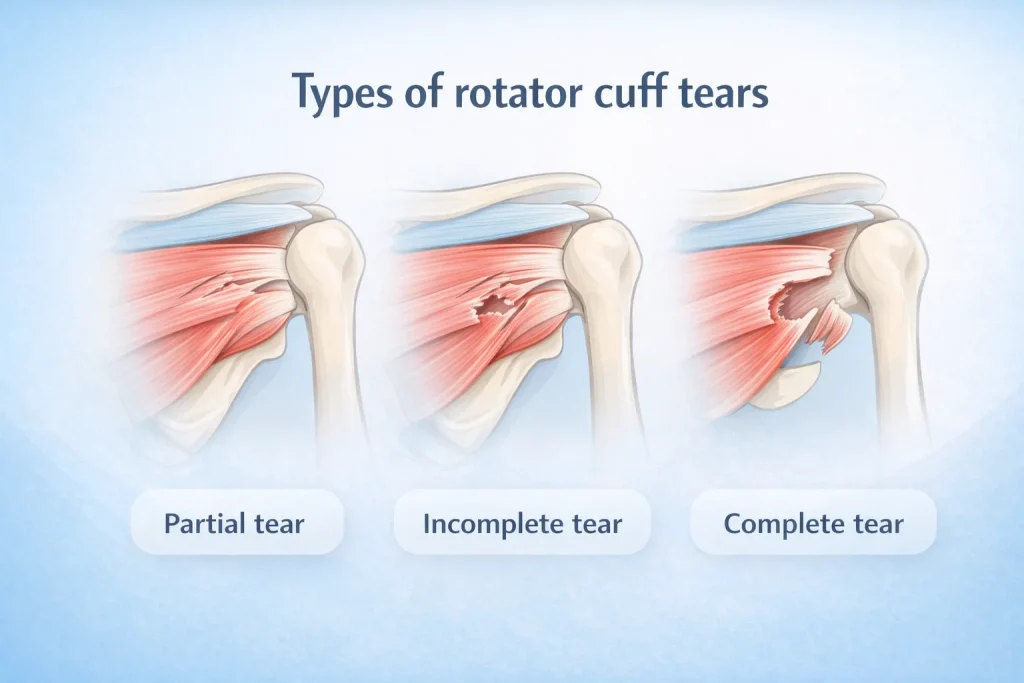
Not all rotator cuff tears are the same. The type of tear you have directly determines your symptoms, what shows up on a rotator cuff tear MRI, and which treatment path is most appropriate for you.
Partial Tear
A partial tear means the tendon is frayed or damaged but has not fully separated from the bone. Think of a rope that is fraying – still holding, but compromised. The tendon is thinner than normal and weaker, but it is still attached.
- Pain is usually present but may come and go
- Arm weakness is mild in most cases
- Many partial rotator cuff tears respond well to non-surgical treatment
Full-Thickness Incomplete Tear
Part of the tendon has detached from the humerus, but the tear does not pass completely through the tendon’s full width. This is more significant than a partial tear and requires careful monitoring and guided treatment.
Full-Thickness Complete Tear
The tendon has fully separated from the bone – there is essentially a hole in the rotator cuff. This is the most severe type and is often visible as cuff tear arthropathy on imaging.
- Arm weakness is significant and often sudden
- Pain is typically severe and does not improve with rest alone
- Surgery is usually recommended, especially in younger or active patients
When classifying rotator cuff tears, surgeons also consider tear size: small (less than 1 cm), medium (1–3 cm), large (3–5 cm), and massive (more than 5 cm). Size directly influences whether the tear is repairable and which surgical technique is best suited.
What Causes a Rotator Cuff Injury?

Rotator cuff injuries have two primary origins – sudden trauma and gradual degeneration. Understanding which applies to you matters because the cause shapes the entire treatment approach.
Acute (Traumatic) Causes
Acute rotator cuff injuries happen in an instant. Common causes include:
- Falling on an outstretched arm
- Lifting a heavy object with a sudden jerking motion
- A direct blow to the shoulder
- A dislocated shoulder or separated shoulder
- A wrist fracture that transmits force up the arm
Acute tears are more common in younger adults and athletes. The pain and weakness are usually immediate and obvious. Terms like pulled shoulder or pulled deltoid are sometimes used informally for milder versions of this type of injury – but any significant sudden shoulder pain should be assessed by a specialist.
Degenerative (Wear-Related) Causes
Most rotator cuff tears are not caused by a dramatic event. They develop gradually over the years as the tendons wear down – a process that accelerates with age and repetitive activity. This is the most common type in adults over 40.
Key contributors to degenerative tears include:
- Repetitive stress – repeating the same overhead or lifting motion daily puts chronic stress on the tendons. Painters, carpenters, electricians, teachers, and athletes who perform overhead actions are especially vulnerable. This repeated mechanical load is the primary driver of rotator cuff syndrome in the working population.
- Reduced blood supply – as we age, blood flow to the critical zone of the supraspinatus tendon decreases. Without good circulation, tendons cannot efficiently repair the micro-damage that accumulates with daily use. This leads to mild tendinosis initially and eventually to a partial or full tear.
- Bone spurs – extra bone growth under the acromion can press against the supraspinatus tendon, gradually abrading it over time.
- Previous shoulder tendon injury – a prior rotator cuff strain or shoulder tendon injury, even a minor one, increases the risk of a future tear.
Risk Factors
- Adults over 40 – the single strongest risk factor for a degenerative rotator cuff tear
- Dominant arm users – tears are significantly more common in the dominant arm
- Athletes – particularly baseball pitchers, tennis players, swimmers, and weightlifters
- Manual labourers – painters, carpenters, electricians, and others who do sustained overhead work
- People with a previous shoulder injury – prior dislocations or shoulder ligament tears, raise the risk considerably
Rotator Cuff Tear Symptoms – How to Know If You Have One
Symptoms differ depending on whether the tear was sudden or developed gradually. Here is what each typically looks and feels like.
Symptoms of an Acute (Sudden) Tear:
- A sharp, intense pain in the shoulder at the moment of injury
- A snapping or tearing sensation is felt inside the shoulder
- Immediate, significant arm weakness – difficulty lifting even light objects
- Swelling and tenderness along the upper arm and outer shoulder
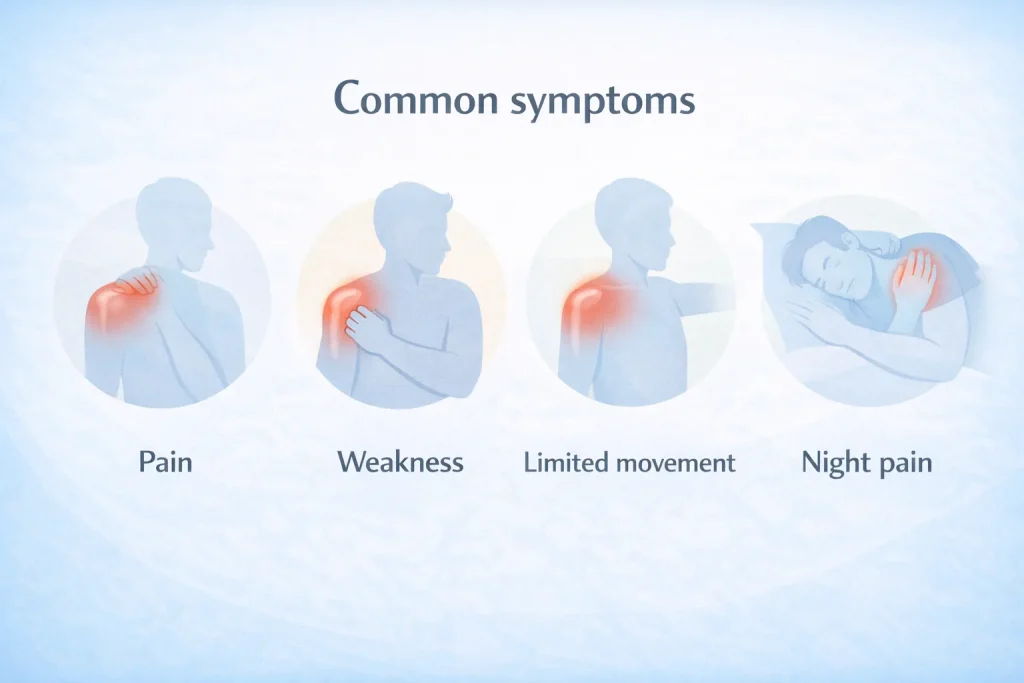
Symptoms of a Gradual (Degenerative) Tear:
- Shoulder pain when lifting the arm overhead or reaching behind the back
- Dull, aching rotator cuff pain that worsens at night, especially when lying on the affected side
- Gradual arm weakness that makes daily tasks like dressing, lifting, or combing hair increasingly difficult
- A crackling or clicking sensation (crepitus) during shoulder movement
- Rotator cuff pain location is typically felt deep inside the shoulder, often radiating down the outer upper arm
One critical point: some rotator cuff tears – especially partial and degenerative ones – cause no pain at all, yet still produce noticeable weakness. Do not use pain as your only indicator that something is wrong. If your shoulder feels weak or limited, get it assessed even if the pain seems manageable.
When to see a specialist – do not delay if you have:
- Sudden severe shoulder pain following a fall or accident
- Inability to raise your arm or reach overhead
- Shoulder tear symptoms that have persisted for more than 4–6 weeks
- Progressive arm weakness, even when pain feels manageable
- Night pain that is consistently disrupting your sleep
How is a Rotator Cuff Tear Diagnosed?

Self-diagnosis is unreliable. Many shoulder conditions – impingement syndrome, frozen shoulder, shoulder ligament tear, rc tendonitis, and rotator cuff tendinosis – share overlapping symptoms with a rotator cuff tear. A precise diagnosis requires clinical assessment by a specialist, combined with appropriate imaging.
Physical Examination and Rotator Cuff Injury Tests
An orthopaedic specialist will begin with a thorough hands-on assessment:
- Range of motion testing – how far and comfortably you can move the arm in each direction
- Strength testing – isolating each tendon’s function through specific arm positions
- Supraspinatus tear test (Empty Can Test) – the arm is held at 90 degrees with the thumb pointing down, and the examiner applies downward resistance. Pain or weakness suggests a supraspinatus injury.
- External rotation lag sign – tests the infraspinatus muscle; an inability to maintain the arm in external rotation points to a significant infraspinatus tear
- Drop Arm Test – the patient raises the arm fully and tries to lower it slowly; inability to do so suggests a full-thickness tear
- Neck examination – to rule out a pinched nerve, which frequently mimics shoulder symptoms and is a common source of diagnostic confusion
Imaging – X-Ray, MRI, and Ultrasound
Physical examination alone cannot confirm the diagnosis or show the tear’s size. Imaging is essential.
- X-Ray (Rotator Cuff Tear X-Ray): Reveals bone structure – rules out arthritis, shoulder fractures, and acromial bone spurs. X-rays cannot show soft tissues like tendons, but they provide important context and can show indirect signs of a long-standing degenerative tear.
- MRI (Rotator Cuff Tear MRI): The gold standard for rotator cuff evaluation. MRI shows the exact location, size, and type of tear; whether it is acute or chronic; the quality of the surrounding rotator cuff muscles; and associated conditions like rotator cuff tendinosis or cuff tear arthropathy. Rotator cuff tear radiology interpretation by a specialist guides the entire surgical or conservative treatment plan.
- Ultrasound: Faster and more accessible than MRI. Useful for identifying shoulder tendon tears in real time during movement. Accuracy depends significantly on the skill of the technician performing the scan.
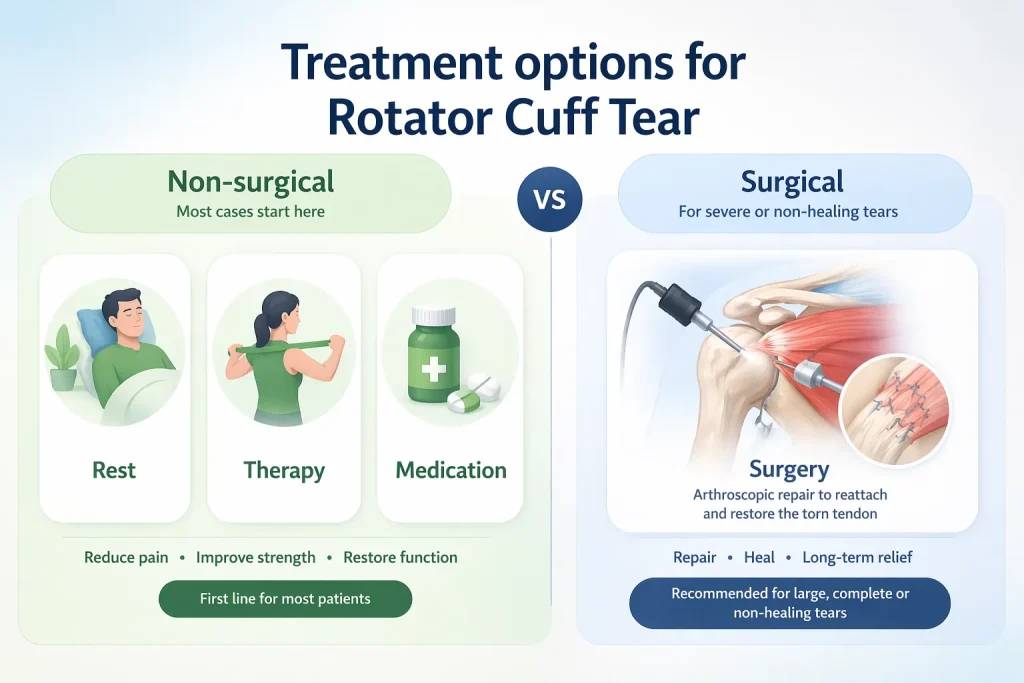
Treatment Options – Non-Surgical and Surgical
Treatment depends on the type and size of the tear, your age, activity level, and the degree of pain and weakness you experience. There is no universal answer – your orthopaedic surgeon will discuss the best approach for your individual situation.
Non-Surgical Treatment
In about 80–85% of patients, non-surgical treatment effectively reduces rotator cuff pain and restores enough shoulder function for daily life. Conservative options include:
- Rest and activity modification – avoiding overhead movements and lifting that aggravate symptoms
- NSAIDs – medications like ibuprofen or naproxen reduce rotator cuff pain and swelling in the short term
- Physical therapy (rotator cuff tear therapy) – targeted exercises to strengthen the remaining healthy cuff muscles, improve shoulder flexibility, and reduce pain without surgery. This is the cornerstone of non-surgical rotator cuff tear treatment and shoulder muscle tear treatment overall.
- Steroid (cortisone) injections – a local anaesthetic combined with cortisone can provide meaningful rotator cuff pain treatment in about two-thirds of patients for at least three months. Not a long-term cure, but valuable in managing acute flare-ups.
The main advantages of non-surgical treatment are avoiding surgical risks – infection, stiffness, anaesthesia complications, and the risk of re-tear. The main disadvantage is that a tear may enlarge over time if the underlying cause is not addressed.
Rotator Cuff Surgery
Your surgeon may recommend rotator cuff surgery if:
- Symptoms persist beyond 6–12 months despite consistent conservative treatment
- The tear is large (more than 3 cm), and the surrounding tissue quality is good
- You have significant arm weakness and loss of shoulder function
- The tear was caused by an acute traumatic injury
- You are young and physically active, with high demands on your shoulders
Surgery most commonly involves reattaching the torn tendon to the head of the humerus. The most widely used approach today is arthroscopic rotator cuff repair – a minimally invasive muscle tear operation performed through small keyhole incisions using a camera and specialised instruments. This reduces recovery time and surgical risk compared to traditional open surgery.
Recovery and Rehabilitation

Recovery from rotator cuff surgery varies by tear size and patient factors, but a general timeline looks like this:
- Weeks 1–6: Arm in a sling; gentle passive movement exercises begin within days to prevent joint stiffness
- Weeks 6–12: Active range-of-motion exercises; sling use gradually phased out
- Months 3–6: Strengthening programme begins; rotator cuff muscles examination shows progressive improvement
- Months 6–12: Return to full activity for most patients; shoulder muscle tear recovery time is longer for larger, more complex tears
Following the prescribed rehabilitation programme consistently is the single most important factor in a successful outcome after rotator cuff repair.
Can a Rotator Cuff Tear Heal Naturally Without Surgery?

This is one of the most common questions patients ask – and the honest answer is: it depends on the type and size of the tear.
- Partial tears – Many partial rotator cuff tears stabilise or improve significantly with proper rest, targeted physical therapy, and activity modification. The body can repair micro-damage given the right conditions and enough time.
- Small full-thickness tears – In some older or less active patients, small full-thickness tears can be managed long-term with conservative care, even without surgical repair.
- Large or complete tears – A full-thickness complete tear rarely heals on its own. Without repair, the tendon continues to retract, and the rotator cuff muscles begin to atrophy. Waiting too long can make the tear irreparable, even with surgery.
If you are exploring how to heal a torn rotator cuff naturally, the honest answer is structured physical therapy, careful load management, and close follow-up with your orthopaedic specialist – not simply resting and hoping. The earlier you get an accurate diagnosis, the more options remain available to you.
Expert Insights – What Most Patients Get Wrong About Rotator Cuff Injuries
Based on orthopaedic practice, these are the most common misconceptions that delay treatment and worsen outcomes:
- “The pain went away, so I must be fine.” Pain reduction does not mean the tear has healed. Rotator cuff disease can progress silently. A 1 cm tear that is manageable today can become a massive, irreparable tear months later.
- “I just pulled my shoulder muscle – I do not need imaging.” A pulled shoulder and a rotator cuff tear can feel nearly identical in the early stages. Only imaging – particularly an MRI – can distinguish between them definitively.
- “Physical therapy did not work, so surgery is my only option.” Physical therapy works best when it is condition-specific and consistently applied for at least three months. Many patients under-commit to the programme or stop when the initial pain reduction plateaus.
- “Surgery means a quick fix.” Rotator cuff surgery is highly effective, but it requires 6–12 months of rehabilitation to achieve full benefit. Treating surgery as the end rather than the beginning of recovery leads to poor outcomes.
- “I am too old for surgery.” Age alone is not a reason to avoid surgery. Tissue quality, activity level, and overall health are far more relevant than age when planning a rotator cuff repair.
Conclusion
A rotator cuff tear is one of the most common and most treatable orthopaedic conditions – if it is caught early and managed correctly.
Here is what you should take away from this guide:
- The rotator cuff is a group of four muscles (the SITS group) whose tendons stabilise and move the shoulder. The supraspinatus is the most commonly torn.
- Tears range from partial (tendon frayed, still attached) to full-thickness complete (total detachment). Treatment depends heavily on the type and size.
- Causes are either acute (sudden trauma) or degenerative (gradual wear). Most tears in adults over 40 are degenerative.
- Symptoms include shoulder pain when lifting the arm, arm weakness, night pain, and crepitus – but some tears are entirely painless. Do not rely on pain as your only indicator.
- Diagnosis requires physical examination combined with imaging – ideally an MRI – for an accurate picture.
- Non-surgical treatment works for the majority of patients. Surgery is reserved for large tears, acute injuries, or cases where conservative management has failed.
- Recovery from surgery takes 6–12 months. Consistent rehabilitation is the single most important factor in outcomes.
- Early assessment gives you more options. Waiting allows tears to progress to a point where repair becomes more complex – or impossible.
If you are experiencing shoulder pain, arm weakness, or any of the symptoms described in this guide, the right first step is a specialist consultation. At deformity.co.in, our orthopaedic team provides precise diagnosis and personalised treatment plans – from conservative management to advanced arthroscopic rotator cuff repair.
FAQs
What is a rotator cuff tear?
A rotator cuff tear is a rupture in one or more of the four tendons surrounding the shoulder joint. It causes pain, weakness, and reduced arm mobility. Nearly 2 million people are diagnosed with this condition every year worldwide.
What are the most common rotator cuff injury symptoms?
The most common symptoms include shoulder pain when lifting the arm, weakness during overhead tasks, night pain on the affected side, and a crackling sensation during shoulder movement. Some tears cause no pain at all.
What causes a rotator cuff injury?
Rotator cuff injuries are caused by either sudden trauma, such as falls or heavy lifting, or gradual degeneration due to age, repetitive overhead activity, or reduced blood supply to the supraspinatus tendon over time.
How is a rotator cuff tear diagnosed?
Diagnosis combines physical examination using specific rotator cuff injury tests such as the Empty Can and Drop Arm tests, with imaging – usually an MRI – which shows tear size, location, and surrounding tissue quality.
Can a rotator cuff tear heal without surgery?
Partial tears often stabilize with physical therapy and rest. Small full-thickness tears may be managed conservatively in older, less active patients. Large, complete tears rarely heal without surgical intervention and repair.
What is the difference between a partial tear and a full-thickness tear?
A partial tear means the tendon is frayed but still attached to the bone. A full-thickness tear means part or all of the tendon has completely detached, creating a hole in the rotator cuff with significant resulting weakness.
How long does recovery from rotator cuff surgery take?
Recovery typically takes 6–12 months. The first 6 weeks involve sling use and passive exercises. Active strengthening begins around 3 months. Full return to overhead sport or heavy labour usually takes 9–12 months.
What is the best treatment for rotator cuff pain?
The best treatment depends on tear severity. Most cases begin with rest, NSAIDs, and physical therapy. Steroid injections help in the short term. Surgery is reserved for large tears or cases where conservative treatment has failed.
What does a rotator cuff tear MRI show?
An MRI reveals the exact location and size of the tear, whether it is partial or full-thickness, the age of the injury, the surrounding muscle quality, and associated conditions like tendinosis or cuff tear arthropathy.
What is a supraspinatus tendon tear, and how is it treated?
A supraspinatus tendon tear is the most common type of rotator cuff tear. Treatment depends on severity – partial tears often respond to physiotherapy, while full-thickness tears in active patients usually require arthroscopic surgical repair.