You reach out to break a fall – and your wrist takes the full impact. In that split second, one of the most common bone injuries in the human body occurs: a distal radius fracture, more widely known as a broken wrist.
Whether you’ve just been diagnosed, are supporting someone through recovery, or want to understand your treatment options before your next appointment, this guide gives you a clear, medically accurate picture of everything involved. From fracture types and X-ray findings to surgical options and recovery timelines, here is what you need to know.
Table of Contents
What is a Distal Radius Fracture?
The forearm has two long bones – the radius and the ulna. The radius sits on the thumb side of the forearm, and the ulna runs along the pinky side. Near the wrist (the distal forearm), the radius is the wider, weight-bearing bone that forms a major part of the wrist joint.
A distal radius fracture occurs when the radius breaks close to its lower end – typically within about 1 inch (2.5 cm) of the wrist joint. This makes it one of the most frequently broken bones in the arm and, in fact, across the entire skeletal system.
Anatomy of the Radius and Ulna
- The proximal forearm (near the elbow) is dominated by the ulna.
- The distal forearm (near the wrist) is dominated by the radius.
- The distal end of the radius connects to the carpal bones, forming the wrist joint.
- The distal end of the ulna (the ulnar styloid) sits alongside, often fractured simultaneously.
Understanding this anatomy helps explain why wrist injuries so frequently involve the distal radius – it is the primary load-bearing surface when the hand meets any force.
Types of Distal Radius Fractures
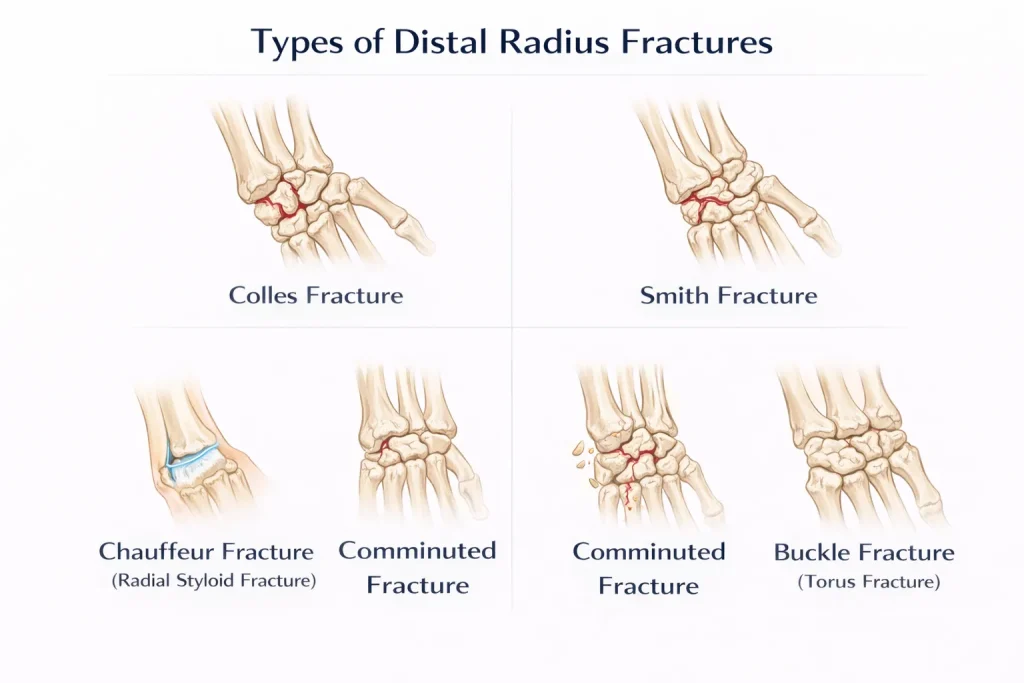
Not all wrist fractures are the same. The location of the break, the direction of bone displacement, and whether the joint surface is involved all define the type – and determine the treatment.
Colles Fracture
The Colles fracture is the most common distal radius fracture. First described in 1814 by Irish surgeon Abraham Colles, it occurs when the broken fragment of the radius tilts upward (dorsally). This creates the classic dinner fork deformity – a visible step-off or bend at the wrist that resembles the shape of a dinner fork when viewed from the side.
- Typically caused by a fall on an outstretched hand (FOOSH mechanism)
- Common in older adults, especially those with osteoporosis
- The Colles fracture displacement involves dorsal angulation and radial shortening
- Treatment depends on severity: cast, closed reduction, or surgery
Smith Fracture
A Smith fracture is the reverse of a Colles fracture. Here, the distal fragment tilts forward (volarly), toward the palm. It is sometimes called a “reverse Colles fracture” and is less common. It often results from a fall on a flexed wrist.
Chauffeur Fracture (Radial Styloid Fracture)
A chauffeur fracture (also called a radial styloid fracture) involves an isolated break of the radial styloid process – the bony projection at the outermost edge of the radius. Historically associated with the backfire of early automobile cranks, it is now seen in sports injuries and motor vehicle accidents.
Intra-Articular vs. Extra-Articular Fracture
This distinction is clinically important:
- Intra-articular fracture: The fracture line extends into the wrist joint surface. These are more complex, require precise alignment, and carry a higher risk of post-traumatic arthritis if not treated correctly.
- Extra-articular fracture: The fracture stays outside the joint. These are generally easier to manage and carry a better prognosis.
The terms intra-articular extension and articular fracture refer to the same concept – joint surface involvement.
Displaced vs. Undisplaced (Non-Displaced) Fracture
- A displaced fracture means the broken bone ends have shifted out of their normal alignment. These often require reduction (realignment).
- An undisplaced fracture (also called a non-displaced or minimally displaced fracture) means the bone has cracked but the pieces remain in their correct position. These are typically managed with casting alone.
- A mildly displaced fracture falls in between – some shift is present but may still be manageable without surgery.
Comminuted Fracture
When the bone shatters into more than two fragments, it is called a comminuted fracture. These are more challenging to treat and more likely to require surgical fixation. They frequently result from high-energy trauma such as road traffic accidents.
Buckle (Torus) Fracture – Common in Children
A torus fracture (buckle fracture) is a type of incomplete fracture where one side of the bone buckles without breaking completely through. It is particularly common in pediatric distal radius fractures because children’s bones are more flexible. These typically heal well with a short period of splinting.
Frykman Classification of Distal Radius Fractures
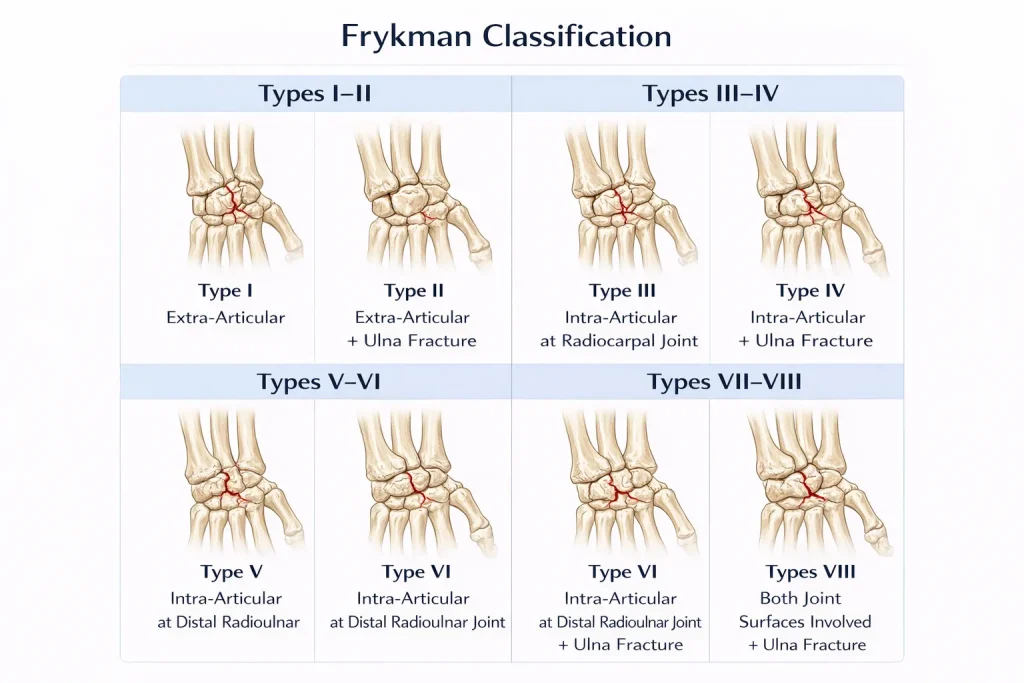
The Frykman classification of distal radius fractures is one of the most widely used systems for categorizing these injuries. It divides fractures into 8 types (Types I–VIII) based on two main factors:
- Whether the fracture is intra-articular or extra-articular
- Whether there is an associated distal ulna fracture
Higher Frykman numbers indicate greater complexity. For example:
- Type I & II: Extra-articular (without/with ulna fracture)
- Type III & IV: Intra-articular at the radiocarpal joint
- Type V & VI: Intra-articular at the distal radioulnar joint
- Type VII & VIII: Both joint surfaces involved
This classification helps surgeons communicate about fracture severity and plan appropriate treatment.
What Causes a Distal Radius Fracture?

Fall on an Outstretched Hand (FOOSH)
The overwhelming majority of distal radius fractures result from a fall on an outstretched hand – a mechanism so common it has its own medical acronym: FOOSH. When you instinctively extend your arm to catch a fall, the full force of impact travels through your palm, up through the wrist, and concentrates at the distal radius.
Osteoporosis and Bone Fragility
Osteoporosis significantly lowers the force required to fracture the distal radius. In patients over 60, a simple fall from standing height can cause a serious wrist fracture – the same fall that might cause only a bruise in a younger, healthier person.
Many wrist fractures in older adults serve as a first warning sign of undiagnosed osteoporosis. Doctors often recommend bone density testing after a distal radius fracture, particularly in postmenopausal women.
High-Energy Trauma
In younger patients with healthy bones, distal radius fractures typically require significant force: car accidents, motorcycle crashes, falls from height, or sports impacts. These injuries are more likely to produce comminuted or open fractures and may involve the radius and ulna fracture simultaneously.
Signs and Symptoms of a Broken Wrist

Recognizing the symptoms of a distal radius fracture early helps ensure timely and appropriate treatment:
- Immediate, intense pain at the wrist after injury
- Swelling and bruising that develops rapidly
- Tenderness when touching the area just above the wrist
- Visible deformity – the wrist may appear bent or misshapen (the classic dinner fork deformity in Colles fractures)
- Restricted movement – difficulty or inability to move the wrist or fingers normally
- Numbness or tingling in the fingers, which may indicate nerve involvement
Important: Numbness or pale fingers after a wrist injury are red-flag symptoms. Seek emergency care immediately. Delayed treatment can result in permanent nerve damage.
How Is a Distal Radius Fracture Diagnosed?
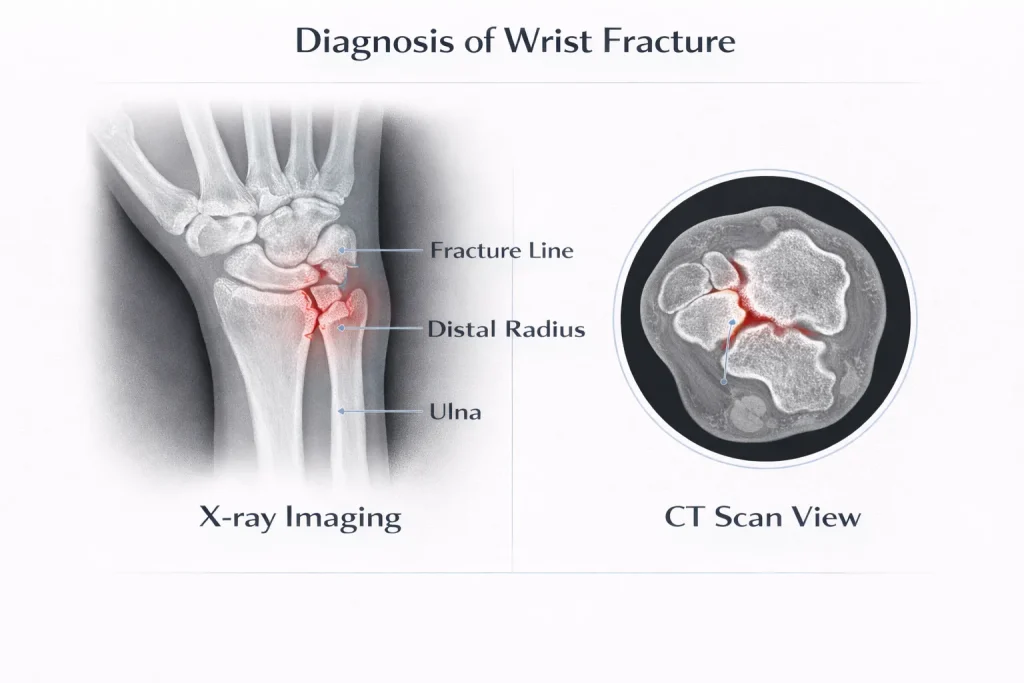
X-Ray of the Wrist
The first and most essential investigation is a wrist X-ray (radius X-ray). It reveals:
- Whether the bone is broken
- The location and direction of the fracture line
- How many fragments exist
- The degree of displacement
- Whether the distal ulna is also fractured
A Colles fracture X-ray characteristically shows dorsal tilt and radial shortening. Understanding wrist X-ray anatomy is essential for accurate interpretation.
CT Scan for Complex Fractures
For intra-articular fractures or cases where surgical planning is needed, a CT scan provides detailed 3D imaging of the distal radius. This helps surgeons assess the exact position of each fragment and plan a fixation strategy with precision.
Distal Radius Fracture Treatment
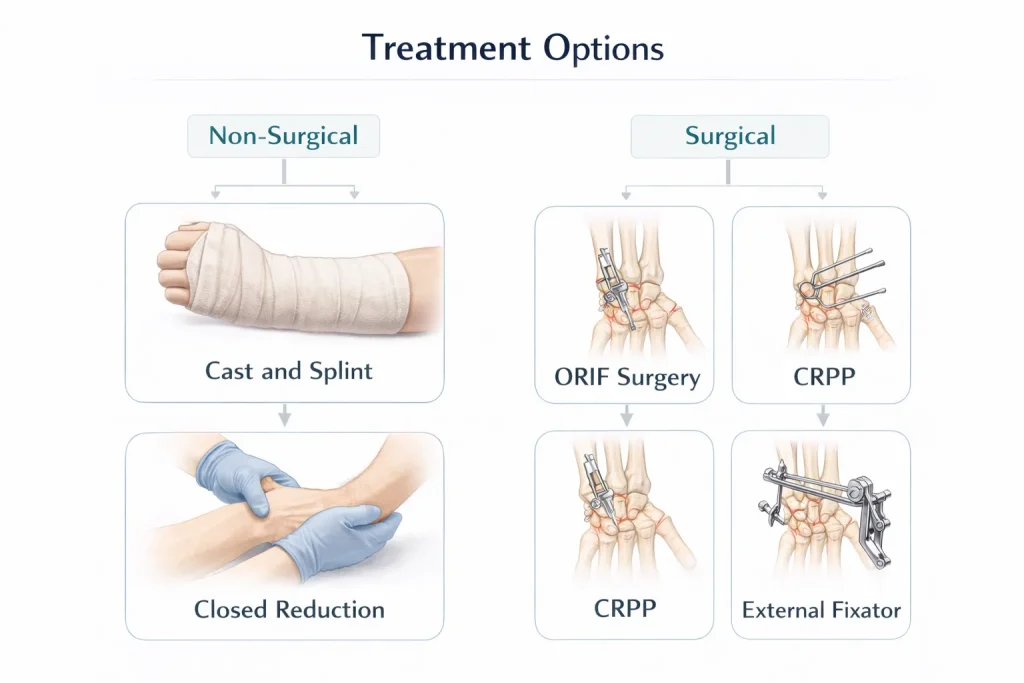
The fundamental goal of treatment is simple: realign the broken bone and hold it in place until it heals. The method chosen depends on the fracture type, the patient’s age and activity level, bone quality, and the surgeon’s assessment.
Non-Surgical Treatment – Cast & Splint
For undisplaced or minimally displaced fractures where the bone is in an acceptable position, a plaster cast or splint is applied:
- A splint is used initially (first few days) to accommodate swelling
- A fractured wrist cast replaces the splint once swelling subsides (usually within a week)
- The cast is typically worn for 6 weeks
- X-rays are repeated at 1, 2, 3, and 6 weeks to monitor alignment
- A wrist fracture bandage or removable splint may be used during rehabilitation
Closed Reduction
When the fracture is displaced but can be corrected without surgery, the doctor performs a closed reduction – manually realigning the broken fragments using controlled manipulation, without making any incision. A Colles fracture reduction is the most frequently performed version of this procedure. After reduction, a Colles fracture cast is applied in the correct position (the Colles fracture cast position typically involves slight flexion and ulnar deviation).
Surgical Treatment – ORIF with Plate and Screws
Open Reduction Internal Fixation (ORIF) is the current gold standard for surgical treatment of unstable or complex distal radius fractures. The surgeon:
- Makes an incision on the wrist (volar approach is most common)
- Directly visualizes and reduces the fracture fragments
- Fixes them in place using a metal plate and screws
DER plating (Distal End Radius plating) is the term used in India and across South Asia to describe this fixation. The full form: DER = Distal End of Radius. This approach offers strong, stable fixation and allows earlier mobilization.
Recovery after broken wrist surgery, plate and screws, typically involves:
- 2–6 weeks in a removable splint
- Early finger movement is encouraged from Day 1
- Physiotherapy starting within 2–6 weeks post-surgery
Patients sometimes ask about the metal plate in the wrist side effects – in most cases, the plate is well tolerated. Some patients request removal if they experience hardware irritation, though this is not routinely necessary.
CRPP (Closed Reduction and Percutaneous Pinning)
CRPP stands for Closed Reduction and Percutaneous Pinning. In this procedure:
- The fracture is reduced (aligned) without opening the skin
- Metal pins (K-wires) are inserted percutaneously (through small punctures) to hold the fragments in place
- A cast is then applied over the pins
This is commonly used in pediatric distal radius fractures and in adults with certain fracture patterns. The pins are usually removed after 4–6 weeks once healing is confirmed.
DER Plating (Distal End Radius Plating)
DER plating is a widely used surgical technique in India for distal radius fractures. The full form of the DER fracture is Distal End Radius fracture. It uses a low-profile locking plate applied to the volar (palm-side) surface of the radius. Key advantages:
- Stable fixation even in osteoporotic bone
- Allows early wrist mobilization
- Reduces the risk of tendon irritation compared to dorsal plates
External Fixator – JESS Fixator
For severe, comminuted, or open fractures – particularly when soft tissue damage is significant – a JESS fixator (Joshi’s External Stabilization System) or another external fixation device may be applied. It holds the bone in alignment using pins placed above and below the fracture, connected by an external frame.
The JESS fixator for distal radius fracture remains a valuable option when:
- The bone is too fragmented for internal plating
- Open wounds need monitoring and access
- Staged treatment is planned (temporary fixation before definitive surgery)
Treatment for Open Fractures
An open fracture (where bone pierces through the skin) is a surgical emergency:
- Surgery is required within 24 hours
- The wound is thoroughly cleaned (debrided) and irrigated
- Antibiotics are started immediately to prevent infection
- Internal or external fixation is applied as appropriate
Distal Radius Fracture Recovery Time

One of the most common questions patients ask: How long will recovery take?
Here is a realistic, stage-by-stage breakdown:
- 0–2 weeks: Pain, swelling management; splint or cast; elevation and ice
- 2–6 weeks: Cast phase; bone begins to consolidate; X-ray monitoring
- 6 weeks: Most non-operative fractures have the cast removed; physiotherapy begins
- 6–12 weeks: Gradual return to light activities; wrist stiffness improves
- 3–6 months: Return to sports, heavy manual work, or demanding activities
- Up to 1 year: Full functional recovery; some residual stiffness is normal
The distal radius fracture recovery time varies by:
- Patient age (younger patients recover faster)
- Fracture complexity (simple undisplaced vs. comminuted intra-articular)
- Treatment method (surgical vs. non-surgical)
- Bone health and osteoporosis status
- Commitment to physiotherapy
Hairline fracture wrist healing time is typically shorter – around 4–6 weeks – since these involve incomplete bone disruption. A hairline fracture wrist may present with more subtle symptoms but still requires immobilization.
Complications of a Distal Radius Fracture
While most distal radius fractures heal without major issues, the following complications can occur:
- Malunion: Fracture heals in a poor position, leading to wrist deformity and functional loss. Corrective osteotomy may be needed.
- Dinner fork deformity (permanent): Occurs when a Colles fracture heals with persistent dorsal tilt. The classic Colles fracture deformity is a visible cosmetic and functional issue.
- Post-traumatic arthritis: More common after intra-articular fractures, where the joint surface does not heal smoothly.
- Complex Regional Pain Syndrome (CRPS): Persistent, severe, burning pain disproportionate to the injury. Requires aggressive treatment, including nerve blocks.
- Stiffness: Almost universal to some degree; most significant improvement occurs in the first 2 years.
- Tendon and nerve injury: The median nerve, radial nerve, and surrounding tendons can be affected by the fracture or surgical intervention.
- Colles fracture complications specifically include carpal tunnel syndrome, rupture of the extensor pollicis longus tendon, and malunion.
Pediatric Distal Radius Fractures
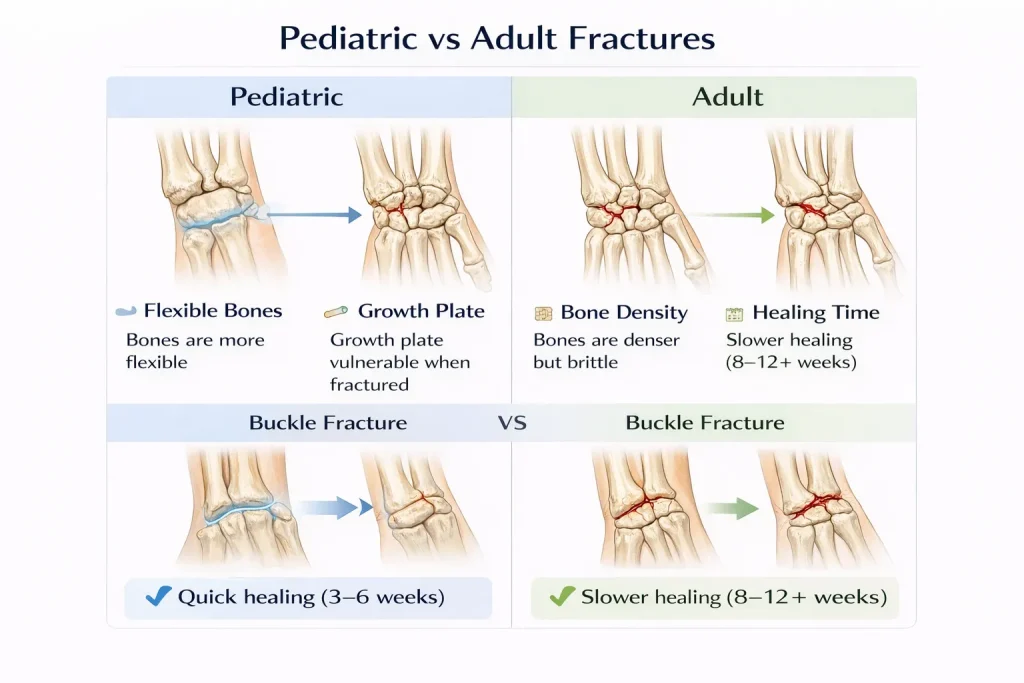
Children’s bones differ from adult bones in important ways. The growth plate (physis) – the area of developing tissue at the end of long bones – is present until adolescence and is a zone of vulnerability.
Key facts about pediatric distal radius fractures:
- Buckle (torus) fractures are the most common type in children
- Growth plate injuries (physeal fractures) require careful evaluation to avoid growth disturbances
- A radius and ulna fracture in a child may be managed with closed reduction under sedation or general anesthesia
- Remodeling – the bone’s ability to straighten itself during growth – allows acceptance of more angulation in children than adults
- Healing is faster in children: cast removal often occurs at 3–4 weeks
Parents should watch for signs of growth disturbance at follow-up appointments, particularly with physeal involvement.
Colles Fracture – A Closer Look
The Colles fracture deserves special attention because it accounts for the majority of distal radius fractures seen in clinical practice – particularly in older women.
Classic features of a Colles fracture:
- Mechanism: FOOSH (fall on an outstretched hand)
- X-ray: Dorsal tilt, radial shortening, loss of radial inclination
- Deformity: Dinner fork appearance
- Associated injury: Ulnar styloid fracture in many cases
Colles fracture management options:
| Severity | Treatment |
| Undisplaced | Below-elbow cast for 6 weeks |
| Displaced, reducible | Closed reduction + Colles cast |
| Unstable / re-displaced | CRPP or DER plating |
| Comminuted | ORIF with locking plate or external fixator |
The Colles fracture splint is used initially and then replaced with a well-moulded cast. The traditional Colles fracture cast position places the wrist in slight palmar flexion and ulnar deviation – though contemporary evidence increasingly favors neutral positioning for better outcomes.
Conclusion
A distal radius fracture – whether a simple undisplaced crack or a complex comminuted intra-articular injury – is one of the most treatable orthopaedic conditions when diagnosed accurately and managed with the right approach.
The key takeaways from this guide:
- The type of fracture – Colles, Smith, intra-articular, displaced, comminuted – directly determines the treatment path. No two wrist fractures are identical.
- Non-surgical treatment with casting and closed reduction works well for stable, undisplaced, or minimally displaced fractures. Consistent X-ray monitoring is essential.
- Surgery – DER plating, CRPP, or ORIF – is indicated when the fracture is unstable, significantly displaced, or involves the joint surface. Modern locking plate systems deliver reliable fixation and allow early wrist movement.
- Recovery is a process, not an event. Most patients regain functional wrist use within 3 months, but full recovery – including resolution of stiffness – can take up to a year.
- Osteoporosis is often the silent factor behind wrist fractures in older adults. A broken wrist should prompt a conversation about bone density testing and long-term bone health.
- Physiotherapy is non-negotiable. Whether treated surgically or conservatively, guided rehabilitation is what restores grip strength, range of motion, and confidence in the wrist.
If you or someone you care for has sustained a wrist injury, early and accurate diagnosis is the single most important step. The difference between a wrist that heals well and one that doesn’t often comes down to the precision of initial treatment decisions.
At deformity.co.in, our team brings together orthopaedic expertise, advanced surgical techniques, and compassionate patient care – because your recovery deserves nothing less than precision at every stage.
FAQs
What is a distal radius fracture?
A distal radius fracture is a break in the radius bone near the wrist, about 1 inch from the joint. It is one of the most common fractures in the arm, often caused by falling on an outstretched hand.
What is the full form of DER fracture?
DER stands for Distal End Radius. A DER fracture refers to a break at the lower end of the radius bone near the wrist, commonly treated with DER plating – a surgical plate-and-screw fixation technique.
What is the difference between a Colles fracture and a Smith fracture?
A Colles fracture tilts the broken bone fragment upward (dorsally), creating a dinner fork deformity. A Smith fracture tilts it forward (volarly). Both involve the distal radius but differ in mechanism and appearance.
How long does a distal radius fracture take to heal?
Most distal radius fractures take 6 weeks in a cast for initial healing. Full functional recovery, including return to all activities, typically takes 3 months to 1 year, depending on fracture complexity and treatment.
What is the difference between intra-articular and extra-articular fractures?
An intra-articular fracture extends into the wrist joint surface, making it more complex to treat. An extra-articular fracture stays outside the joint and generally has a simpler treatment course and better prognosis.
When is surgery needed for a broken wrist?
Surgery is required when the fracture is significantly displaced, unstable, intra-articular, or cannot be maintained in alignment with casting. Options include ORIF with plates, CRPP with pins, or external fixation using a JESS fixator.
What is CRPP in wrist fracture treatment?
CRPP stands for Closed Reduction and Percutaneous Pinning. The fracture is realigned without opening the skin, then held in place by pins inserted through small punctures. A cast is applied afterward, and pins are removed after 4–6 weeks.
What causes a distal radius fracture in older adults?
In older adults, osteoporosis weakens the radius bone, making it vulnerable to fracture even from a minor fall. Many patients over 60 sustain a distal radius fracture from a simple standing-height fall due to reduced bone density.
What is the Frykman classification of distal radius fractures?
The Frykman classification divides distal radius fractures into 8 types based on joint involvement (intra vs. extra-articular) and whether the distal ulna is fractured. Higher numbers indicate greater complexity and typically more challenging treatment.
What is dinner fork deformity in a Colles fracture?
Dinner fork deformity is the visible step-off or bend at the wrist seen in a Colles fracture. The dorsally displaced bone fragment creates a shape resembling a dinner fork when viewed from the side – a hallmark sign of this injury.