Key Takeaways
- A lateral malleolus fracture is the most common ankle fracture worldwide and involves a break in the outer fibula bone.
- Fracture stability is the single most important factor that determines whether a lateral malleolus fracture needs surgery or conservative treatment.
- Even 1 mm of talar shift increases ankle cartilage stress by 42 percent, significantly raising the long-term risk of arthritis.
- Hairline stress fractures of the lateral malleolus are frequently missed on initial X-rays and require MRI or CT for accurate diagnosis.
- Nondisplaced lateral malleolus fractures heal well in a walking boot within 6 to 8 weeks without requiring any surgical intervention.
- The mortise view X-ray is the most critical imaging projection for assessing ankle joint stability after a lateral malleolus fracture.
- Walking too early on an unstable or surgically repaired fracture risks displacement, hardware failure, and significantly delayed bone healing outcomes.
- Weber B fractures at the syndesmosis level require stress X-ray testing because some are stable while others need immediate surgical fixation.
- Bruising spreading toward the inner ankle after a lateral malleolus fracture may indicate ligament injury or a bimalleolar fracture requiring urgent evaluation.
- Full recovery including strength, balance, and return to sport typically takes 3 to 6 months depending on fracture severity and rehabilitation commitment.
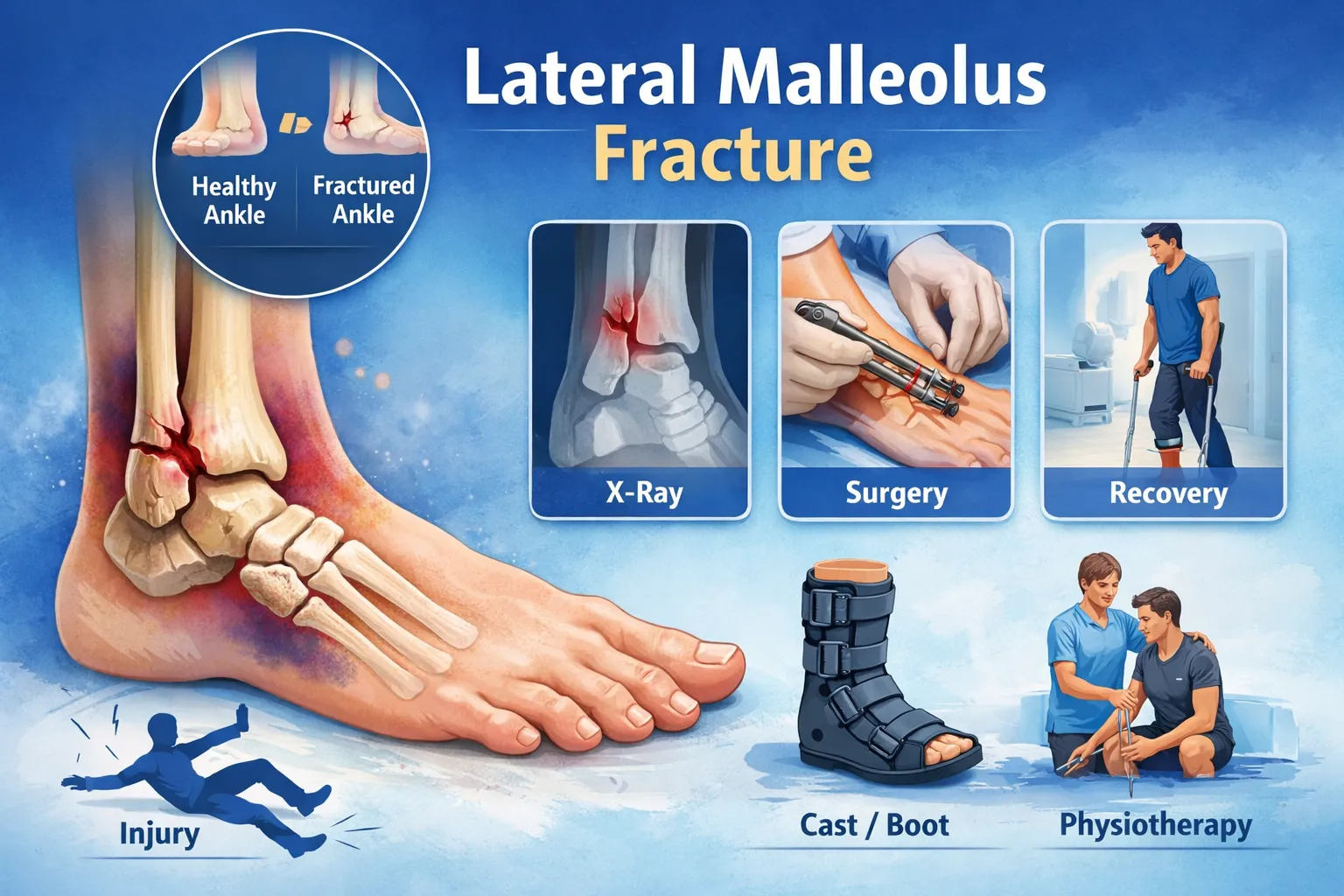
A lateral malleolus fracture is one of the most common ankle injuries worldwide. It involves a break in the outer part of the ankle, specifically the lower end of the fibula (distal fibula). While many lateral malleolus fractures are stable and heal with a cast or walking boot, others can destabilize the ankle joint and require surgical fixation to restore proper alignment and prevent long-term complications like arthritis or chronic instability.
This detailed guide explains everything about lateral malleolus fractures – causes, types, diagnosis, treatment options, recovery timeline, and when surgery is needed. The content is designed for both patients and medical readers globally.
Table of Contents
What is a Lateral Malleolus Fracture?

The lateral malleolus is the bony prominence on the outer side of your ankle. It is the lower end of the fibula and plays a crucial role in stabilizing the ankle joint. A fracture here is often referred to as a distal fibula fracture or outer ankle fracture.
This injury can occur in isolation or along with other ankle fractures, such as medial malleolus or posterior malleolus fractures. The severity depends on whether the fracture affects ankle stability or involves ligament damage.
Key points:
- The most common type of ankle fracture
- Often caused by twisting injuries
- May be stable or unstable
- Stability determines treatment approach
Even a small displacement in the fibula can disrupt ankle mechanics and lead to long-term problems if not treated properly.
Anatomy of the Lateral Malleolus
The lateral malleolus is part of the distal fibula and forms the outer boundary of the ankle joint. It works together with the tibia and talus to create the ankle mortise, which allows smooth movement and weight-bearing.
Important structures attached here include:
- Anterior talofibular ligament (ATFL)
- Calcaneofibular ligament (CFL)
- Syndesmotic ligaments
- Peroneal tendons
Functions of the lateral malleolus:
- Maintains ankle alignment
- Prevents outward shift of the talus
- Provides ligament support
- Stabilizes the ankle during walking and running
Because of its stabilizing role, fractures here must be evaluated carefully to determine whether the ankle joint remains stable.
Causes of Lateral Malleolus Fracture
Lateral malleolus fractures commonly result from twisting or rotational forces applied to the ankle. These injuries are seen across all age groups.
Common causes include:
- Sudden ankle inversion (rolling ankle outward)
- Sports injuries
- Slip and fall accidents
- Road traffic accidents
- Fall from height
- Osteoporosis-related fractures in the elderly
Athletes often sustain these injuries during sudden direction changes, while older adults may fracture the distal fibula after minor falls due to weaker bones.
Mechanism of Injury
Understanding the mechanism helps determine fracture severity and treatment.
Most lateral malleolus fractures occur due to:
- Supination-external rotation injury
- Inversion injury
- Twisting motion while the foot is planted
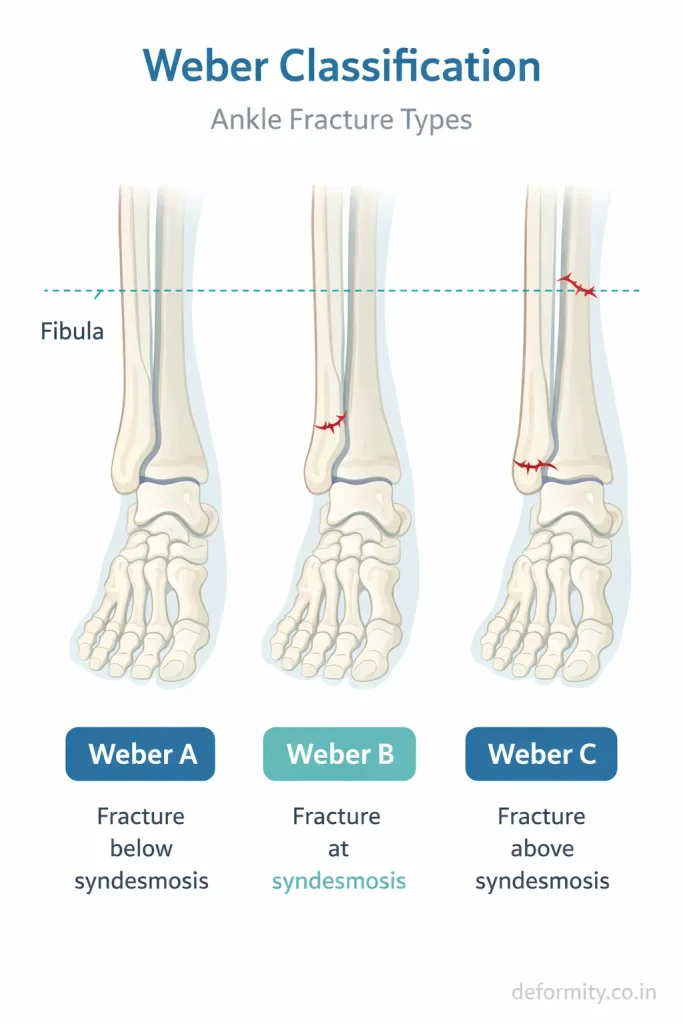
These forces can cause a fracture at different levels of the fibula, which is why classification systems like the Weber classification are important.
Types of Lateral Malleolus Fractures
Lateral malleolus fractures vary in pattern and stability. The treatment depends heavily on the fracture type.
Avulsion Fracture
A small fragment of bone is pulled off by a ligament. Often stable and may heal with conservative treatment.
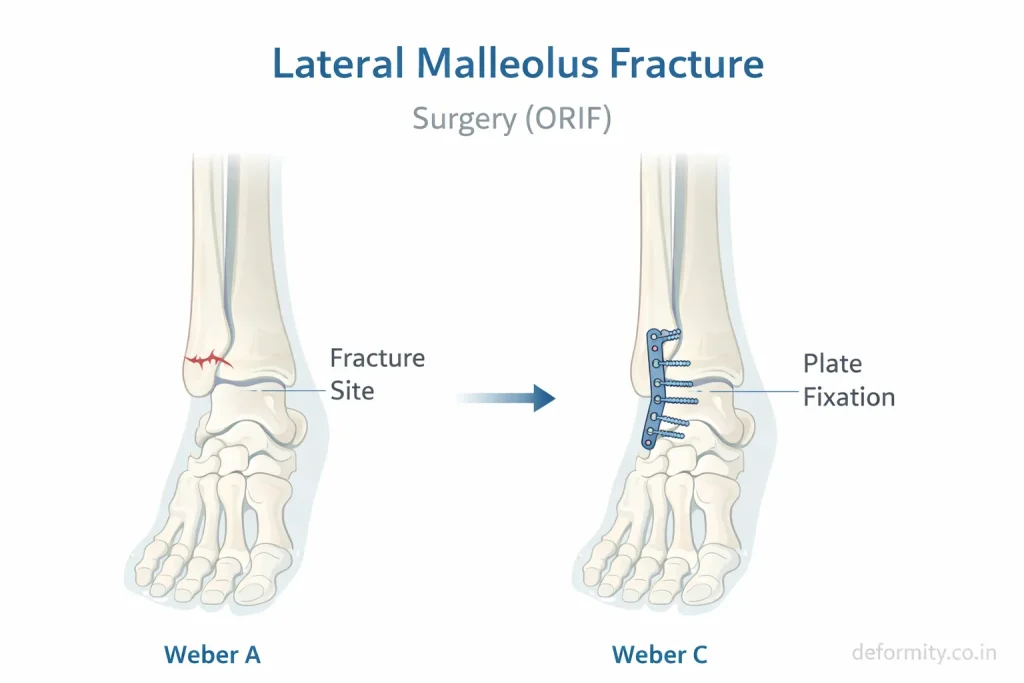
Weber A Fracture
Fracture below the syndesmosis. Usually stable and treated without surgery.
Weber B Fracture
Fracture at the level of the syndesmosis. Stability varies and requires careful assessment. Some cases need surgery.
Weber C Fracture
Fracture above the syndesmosis. Usually unstable and associated with ligament injury. Surgery is often required.
Comminuted Fracture
The bone breaks into multiple fragments. Often unstable and requires surgical fixation.
Spiral Fracture
Caused by twisting force. May be stable or unstable depending on the displacement.
Hairline Fracture of the Lateral Malleolus
A hairline fracture – also called a stress fracture of the lateral malleolus – is a thin, incomplete crack in the bone without significant displacement. It is one of the most commonly missed ankle injuries on initial X-rays and may require an MRI or CT scan for confirmation.
Key features include:
- Gradual onset of outer ankle pain, especially during weight-bearing activity
- No visible deformity and only mild swelling
- Pinpoint tenderness over the fibula on palpation
- Common in runners, dancers, and military recruits due to repetitive stress
Recovery time for a lateral malleolus hairline fracture is typically 6 to 8 weeks with protected weight-bearing and activity modification. Continuing to load the bone without treatment can convert a hairline fracture into a completely displaced fracture requiring surgery.
Nondisplaced Lateral Malleolus Fracture
A nondisplaced fracture means the bone is cracked, but the fragments remain in correct alignment. These are almost always stable and respond well to conservative treatment without surgery.
Typical management includes:
- Walking boot or short leg cast for 4 to 6 weeks
- Protected weight-bearing as tolerated
- Serial X-rays every 1 to 2 weeks to confirm maintained alignment
Nondisplaced lateral malleolus fracture recovery time is generally 6 to 8 weeks for bone healing, and up to 10 to 12 weeks for full functional recovery, including return to sports.
Symptoms of Lateral Malleolus Fracture
Symptoms vary depending on severity and displacement.
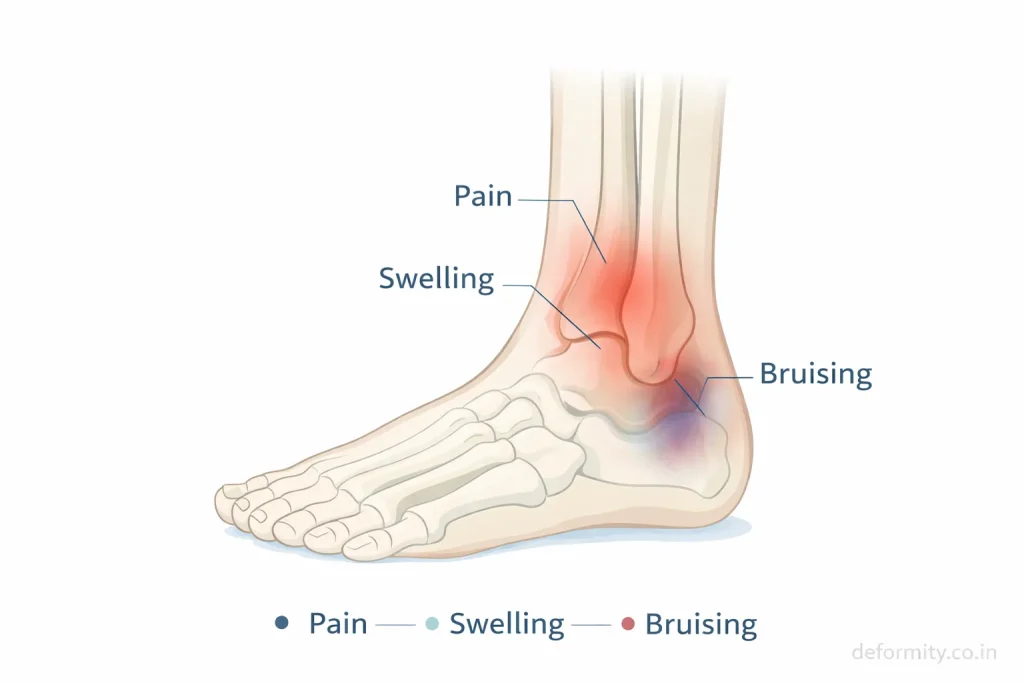
Common symptoms include:
- Pain on the outer side of the ankle
- Swelling around the ankle
- Bruising
- Difficulty bearing weight
- Tenderness over the fibula
- Reduced ankle movement
Severe fractures may cause deformity or inability to stand. Persistent pain after ankle injury should always be evaluated with imaging.
Lateral Malleolus Fracture Bruising and Swelling
Lateral malleolus fracture, bruising and swelling are important clinical signs that help assess the severity of injury. Bruising (ecchymosis) typically appears within 24 to 48 hours and often spreads below the ankle and along the foot due to gravity. Significant bruising extending toward the inner ankle may indicate ligament involvement or a bimalleolar injury and warrants urgent evaluation.
Swelling over the lateral malleolus occurs due to soft tissue damage and bleeding around the fracture site. Most swelling reduces within 2 to 3 weeks, but residual puffiness around the ankle can persist for 3 to 6 months – particularly after displaced or surgically treated fractures. Elevation, ice packs, and compression bandaging are effective tools for controlling early swelling and pain.
Diagnosis
Accurate diagnosis is essential for determining stability and treatment.
Physical Examination
An orthopedic specialist assesses:
- Tenderness over the fibula
- Swelling
- Deformity
- Ability to bear weight
- Ligament stability
X-ray Imaging
X-rays are the primary diagnostic tool. Standard views include:
- AP view
- Lateral view
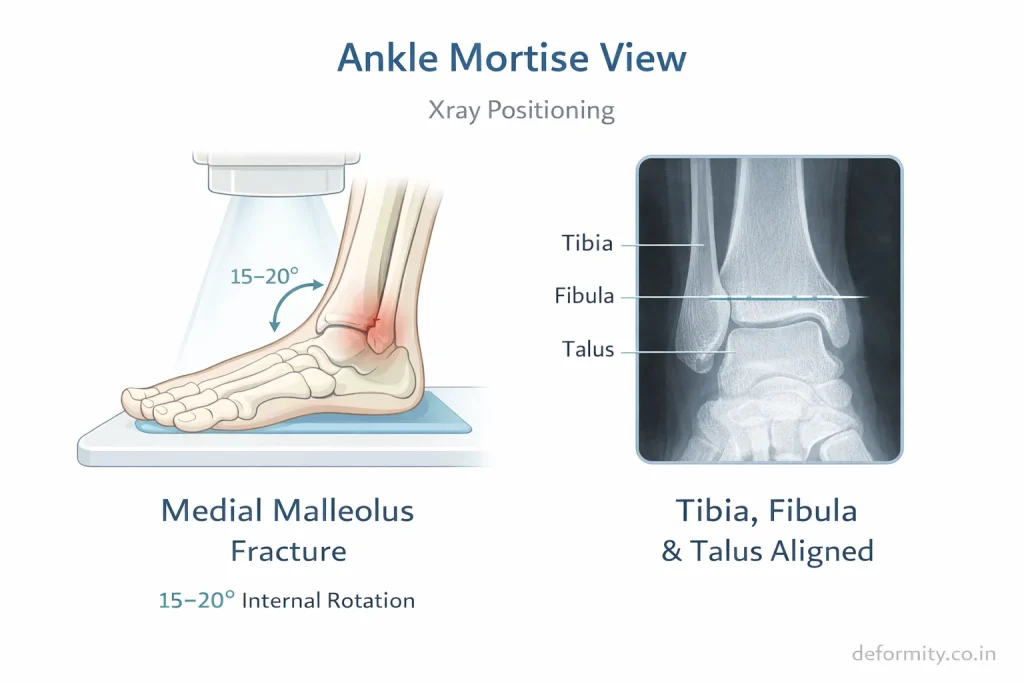
- Mortise view
These help identify fracture pattern and displacement.
What Does a Lateral Malleolus Fracture Look Like on X-ray?
On a lateral malleolus fracture X-ray, the break typically appears as a radiolucent (dark) line through the distal fibula. The exact appearance varies by fracture type:
- Avulsion fracture: A small bone chip near the tip of the lateral malleolus, pulled away by the ATFL or CFL ligament
- Transverse fracture: A horizontal break across the fibula, usually at or below the syndesmosis (Weber A or B)
- Oblique fracture: A diagonal line through the fibula, common in Weber B injuries from external rotation forces
- Spiral fracture: A helical pattern visible across multiple X-ray views
- Comminuted fracture: Multiple fragments without a single clean fracture line
The mortise view is the most critical X-ray projection. It is taken with the ankle in 15 to 20 degrees of internal rotation, allowing the surgeon to assess the ankle joint space uniformly on all sides. Widening of the medial clear space (greater than 4 mm) on the mortise view indicates talar shift – a sign of ankle instability requiring surgical treatment.
Hairline fractures are often invisible on initial plain X-rays. When clinical suspicion is high, an MRI or CT scan is recommended for accurate diagnosis.
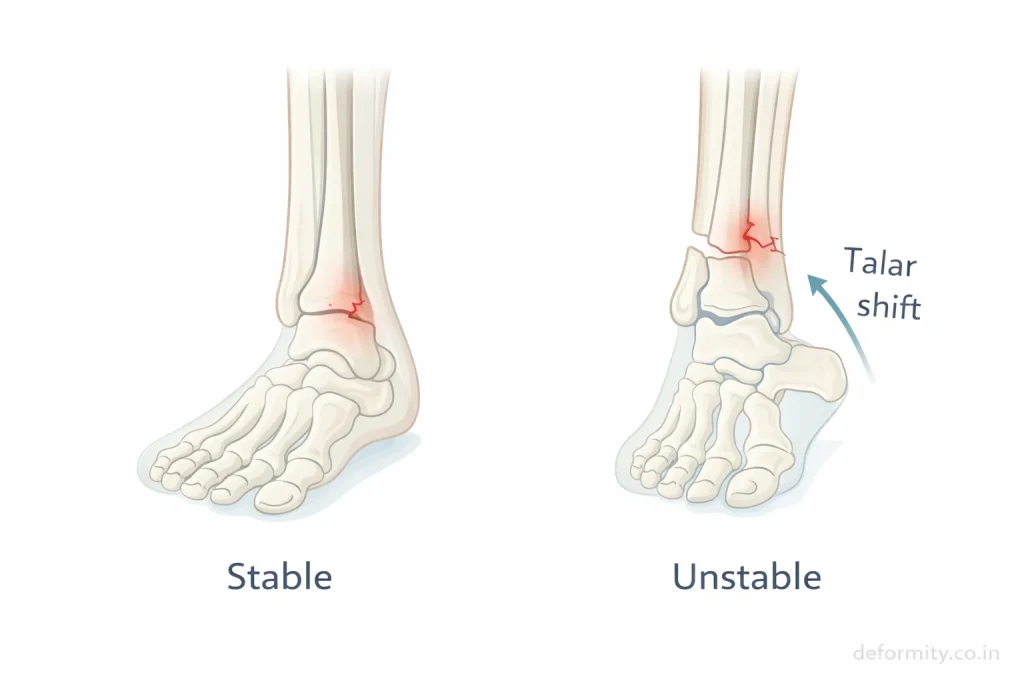
What is Talar Shift and Why Does it Matter?
Talar shift refers to the lateral (outward) displacement of the talus within the ankle mortise. Even a 1 mm shift increases contact stress on ankle joint cartilage by up to 42%, significantly raising the long-term risk of post-traumatic arthritis.
Talar shift is identified on the mortise view X-ray by measuring the medial clear space – the gap between the inner surface of the talus and the medial malleolus. A measurement greater than 4 mm, or greater than the superior clear space, confirms instability that requires surgical correction.
This is why accurate X-ray assessment is critical for every lateral malleolus fracture, even those that appear minor on initial inspection.
CT Scan
A CT scan may be needed when:
- Fracture pattern is complex
- Posterior malleolus involved
- Surgical planning required
Advanced imaging helps determine whether surgery is needed.
Stable vs Unstable Lateral Malleolus Fracture
The most important factor in treatment planning is stability.
A fracture is stable if:
- Bone alignment maintained
- No talar shift
- Ligaments intact
A fracture is unstable if:
- Bone displaced
- Syndesmotic injury present
- Associated medial malleolus fracture
- Joint misalignment
Stable fractures can heal with casting or boot immobilization, while unstable fractures usually require surgical fixation.
Treatment of Lateral Malleolus Fracture
Treatment depends on fracture type, stability, and patient activity level.
Non-Surgical Treatment
Stable fractures can be treated conservatively.
Treatment includes:
- Walking boot or cast
- Rest and elevation
- Ice therapy
- Pain medication
- Follow-up X-rays
- Gradual weight-bearing
Many isolated distal fibula fractures heal well without surgery.
Walking Boot vs Cast for Lateral Malleolus Fracture
One of the most common questions patients ask is whether they need a cast or a walking boot. The decision depends on fracture stability and patient compliance.
A walking boot (removable CAM boot) is preferred for the most stable lateral malleolus fractures because:
- It allows skin inspection and hygiene
- It permits gentle range-of-motion exercises when directed by the surgeon
- It is more comfortable for long-term use
- It enables graduated weight-bearing
A traditional cast may be chosen when:
- The patient is unlikely to comply with boot restrictions
- There is mild displacement that needs firmer immobilisation
- Swelling is significant, and a custom fit is needed
In both cases, the patient must follow weight-bearing restrictions exactly as instructed. Premature full weight-bearing without medical clearance can cause fracture displacement, even in initially stable injuries.
Surgical Treatment (ORIF)
Surgery is recommended when:
- Fracture displaced
- Joint unstable
- Syndesmotic injury present
- Associated fractures exist
The procedure involves:
- Realigning bone
- Plate and screw fixation
- Restoring joint alignment
Surgery helps maintain ankle stability and reduces the risk of arthritis.
Dr Divya Ahuja specializes in advanced fixation techniques designed to restore ankle mechanics and enable early rehabilitation.
ORIF for Lateral Malleolus Fracture – What to Expect
Open Reduction and Internal Fixation (ORIF) is the standard surgical procedure for unstable lateral malleolus fractures. Here is what the process involves:
Before surgery: Pre-operative imaging (X-ray and CT scan) is used to plan the fixation strategy. Swelling is typically managed first with elevation and ice for 5 to 10 days before surgery is performed, as operating on a very swollen ankle increases wound complication risk.
During surgery: The surgeon makes a small incision along the outer ankle to expose the fibula. The fractured fragments are carefully realigned (reduction) and held in place using a plate fixed with screws along the fibula. If the syndesmosis is injured (Weber C pattern), additional syndesmotic screws or a tightrope device may be placed to restore the joint.
After surgery: The ankle is placed in a splint initially. Weight-bearing restrictions vary – typically non-weight-bearing for the first 2 to 6 weeks, followed by gradual progression in a boot. Hardware (plate and screws) is usually left in permanently unless it causes irritation.
Most patients report a significant reduction in pain within 3 to 4 weeks of surgery. Full recovery and return to sport typically takes 3 to 6 months.
Weight Bearing After Lateral Malleolus Fracture
One of the most frequently searched questions is when patients can bear weight after a lateral malleolus fracture. The answer depends entirely on fracture stability and whether surgery was performed.
Non-surgical (stable fractures):
- Immediate protected weight-bearing in a boot is often permitted for truly stable, nondisplaced fractures
- Full weight-bearing is typically allowed at 4 to 6 weeks once X-rays confirm maintained alignment
- Patients should never progress to weight-bearing without their surgeon’s clearance
After surgical fixation (ORIF):
- Non-weight-bearing for the first 2 to 6 weeks is standard
- Partial weight-bearing in a boot begins once early bone healing is confirmed on X-ray
- Full weight-bearing usually resumes at 8 to 10 weeks post-surgery
Walking too early on an unstable or surgically repaired fracture risks displacement, hardware failure, and delayed healing. Always follow the specific protocol provided by your orthopaedic surgeon.
Recovery Time After Lateral Malleolus Fracture
Recovery varies based on severity and treatment.
| Fracture Type | Weight Bearing | Full Recovery |
|---|---|---|
| Stable fracture | 4–6 weeks | 8–10 weeks |
| Surgical fixation | 6–8 weeks | 3–4 months |
| Complex fracture | 8–10 weeks | 4–6 months |
Recovery stages include:
- Swelling reduction
- Bone healing
- Physiotherapy
- Strength rebuilding
- Return to activity
Swelling may persist for several months even after bone healing.
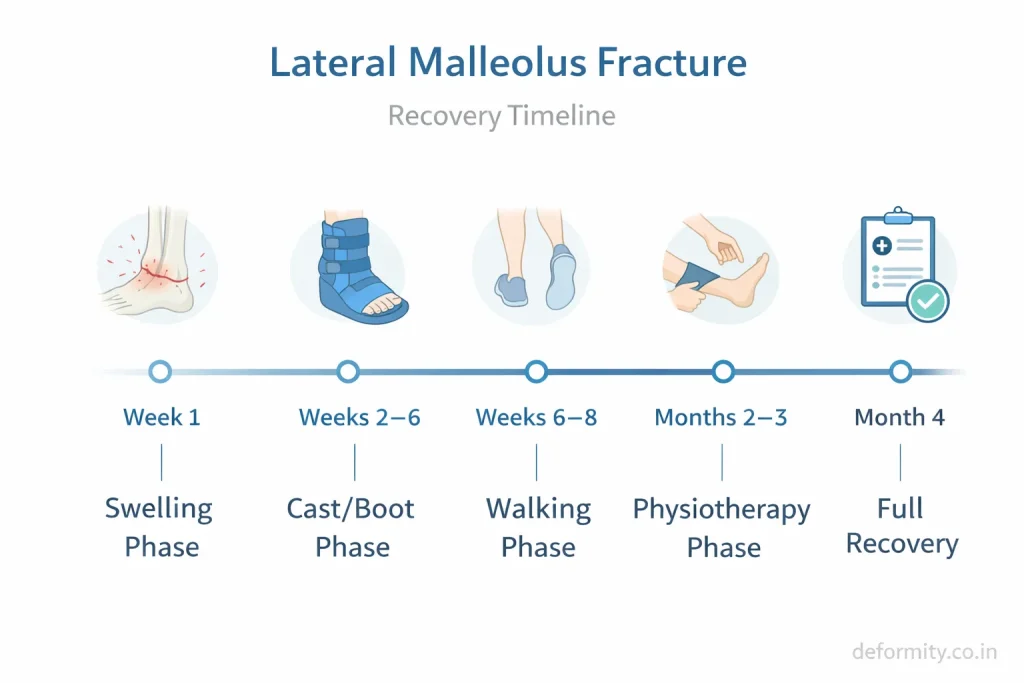
Lateral Malleolus Fracture Healing Stages
Understanding the stages of healing helps patients set realistic expectations and follow their rehabilitation plan effectively.
Stage 1 – Inflammatory phase (Week 1 to 2): The body responds to the fracture with swelling, bruising, and pain. Blood clots form around the fracture site as the first step in healing. Immobilisation and elevation are critical during this stage.
Stage 2 – Soft callus formation (Week 2 to 6): New soft tissue (callus) bridges the fracture gap. The bone is still fragile. X-rays may show early callus formation, but the fracture line remains visible. Weight-bearing is restricted or carefully controlled.
Stage 3 – Hard callus formation (Week 6 to 12): The soft callus is converted into harder woven bone. The fracture line begins to disappear on X-ray. Protected weight-bearing progresses. Physiotherapy begins actively.
Stage 4 – Bone remodelling (Month 3 to 12+): The new bone is reshaped and strengthened along lines of mechanical stress. Pain resolves. Strength and balance are restored through rehabilitation. Return to full activity is possible by months 3 to 6 for most patients.
Rehabilitation & Physiotherapy
Rehabilitation is essential for restoring strength and mobility.
Key components include:
- Range of motion exercises
- Strength training
- Balance exercises
- Gait training
- Return-to-sport conditioning
Skipping physiotherapy may result in stiffness and weakness.
Complications
If not treated properly, complications may occur.
Possible complications include:
- Malunion
- Nonunion
- Chronic ankle instability
- Post-traumatic arthritis
- Stiffness
- Hardware irritation
Proper alignment and rehabilitation reduce long-term risks.
Lateral vs Medial Malleolus Fracture
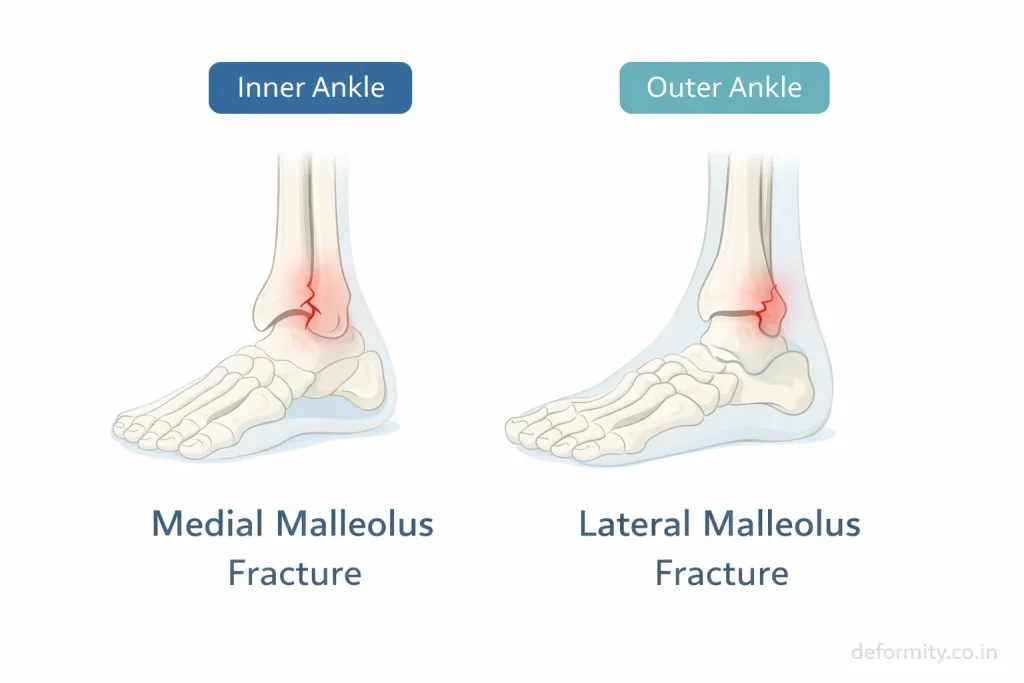
Both fractures affect ankle stability but differ in location and treatment approach.
- Lateral malleolus fracture → outer ankle
- Medial malleolus fracture → inner ankle
- Combined fractures → often unstable
Bimalleolar and Potts Fracture – How They Relate
When both the lateral malleolus and the medial malleolus are fractured together, the injury is called a bimalleolar fracture. When the posterior malleolus (back of the tibia) is also involved, it becomes a trimalleolar fracture – one of the most severe ankle fracture patterns.
A Potts fracture is a historical term that originally described a bimalleolar ankle fracture, named after the English surgeon Percivall Pott. While the term is still occasionally used in clinical settings, modern classification systems (Weber and Lauge-Hansen) are now preferred for guiding treatment.
Bimalleolar and trimalleolar fractures almost always require surgical fixation because both primary stabilisers of the ankle joint are compromised, leading to gross instability and talar shift.
Know more about: Medial Malleolus Fracture
When to See an Orthopedic Surgeon
Seek medical attention if:
- Severe ankle pain persists
- Swelling worsens
- Cannot bear weight
- Deformity visible
- Injury after a fall or twist
Early diagnosis improves healing outcomes.
Treatment in India & International Consultation
Many global patients seek ankle fracture treatment in India due to high-quality care and affordability.
Dr Divya Ahuja provides advanced care for:
- Distal fibula fractures
- Complex ankle injuries
- Sports trauma
- Revision surgeries
International patients benefit from:
- Online consultation
- Treatment planning
- Affordable surgery
- Post-operative rehabilitation
Early expert care ensures better alignment, faster recovery, and long-term joint health.
Conclusion
A lateral malleolus fracture is one of the most common ankle injuries, but it should never be underestimated. Proper evaluation, accurate diagnosis, and appropriate treatment are essential for restoring ankle stability and preventing long-term complications. With timely care and structured rehabilitation, most patients recover well and return to normal activities.
Explore all our fracture-related blogs
| Topic | Link |
| Cervical Radiculopathy | Click here |
| Distal Radius Fracture | Click here |
| Proximal Humerus Fracture | Click here |
| Lauge-Hansen Classification of Ankle Fractures | Click here |
| Weber Classification of Ankle Fractures | Click here |
| Trimalleolar Fracture | Click here |
| Bimalleolar Ankle Fracture | Click here |
| Lateral Malleolus Fracture | Click here |
| Medial Malleolus Fracture | Click here |
| Complete Guide to Ankle Fractures | Click here |
| Femur Shaft Fractures | Click here |
| Tibia Fracture | Click here |
FAQs
How long does a lateral malleolus fracture take to heal?
A lateral malleolus fracture typically heals in 6–8 weeks if stable and treated conservatively. However, full recovery, including strength and mobility, may take 3–4 months, especially if surgery is required or if the fracture is unstable.
Can you walk on a lateral malleolus fracture?
Walking depends on fracture stability. Stable fractures may allow protected weight-bearing in a boot, while unstable fractures require immobilization or surgery. Walking too early without medical advice can worsen displacement and delay healing.
What is the recovery time for a distal fibula fracture?
Recovery from a distal fibula fracture usually takes 8–12 weeks for basic healing. Patients who undergo surgery may require 3–4 months before returning to full activity, depending on rehabilitation progress and fracture severity.
Does a Weber B fracture always need surgery?
Not all Weber B fractures require surgery. If the fracture is stable and there is no talar shift or ligament injury, conservative treatment may be sufficient. Unstable Weber B fractures often need surgical fixation to restore alignment.
How long does swelling last after a lateral malleolus fracture?
Swelling usually improves within 2–3 weeks, but mild swelling may persist for several months. Elevation, compression, and physiotherapy help reduce swelling and improve circulation during the healing process.
Can a lateral malleolus fracture heal without a cast?
Some stable fractures can be managed with a removable walking boot instead of a traditional cast. However, immobilization is still required to ensure proper bone healing and prevent displacement.
When can I drive after a lateral malleolus fracture?
Driving is generally safe once full weight-bearing is possible and reaction time is normal, usually around 6–8 weeks after injury. Right-sided fractures may require a longer recovery before driving is recommended.
What happens if a lateral malleolus fracture is left untreated?
Untreated fractures may heal improperly, leading to ankle instability, chronic pain, or early arthritis. Proper diagnosis and alignment are essential to maintain long-term joint function.
Is surgery painful for distal fibula fractures?
Surgery is performed under anesthesia, so patients do not feel pain during the procedure. Postoperative discomfort is manageable with medication, and most patients report gradual pain reduction within weeks.
How soon can I return to sports after a lateral malleolus fracture?
Return to sports typically occurs 3–6 months after injury, depending on fracture severity and rehabilitation progress. Full strength, balance, and range of motion must be restored before resuming athletic activity.
What is a nondisplaced lateral malleolus fracture, and does it need surgery?
A nondisplaced fracture means the bone is cracked but remains in correct alignment. These fractures rarely require surgery and are treated with a walking boot or cast for 4 to 6 weeks, followed by physiotherapy. Recovery time is typically 8 to 10 weeks.
Is a lateral malleolus fracture the same as a distal fibula fracture?
Yes. The lateral malleolus is the lower end of the fibula, so a lateral malleolus fracture and a distal fibula fracture refer to the same injury. The terms are used interchangeably in clinical practice.
What does a lateral malleolus stress fracture feel like?
A stress fracture of the lateral malleolus causes gradually worsening outer ankle pain during activity, which improves with rest. Unlike an acute fracture from trauma, there is usually no specific injury event. It is common in athletes who increase training load rapidly. MRI is the most accurate diagnostic tool when X-rays appear normal.