Key Takeaways:
- A bimalleolar ankle fracture means both the inner and outer ankle bones are broken, making the joint highly unstable.
- Most bimalleolar fractures require surgery because two broken bones eliminate the structural support the ankle needs for weight bearing.
- A bimalleolar equivalent fracture involves a fibula break plus a torn deltoid ligament, creating the same instability as two bone fractures.
- Displaced bimalleolar fractures require surgical ORIF fixation to realign bones and prevent long-term arthritis or chronic ankle instability.
- Even non-displaced bimalleolar fractures need close monitoring because the underlying instability can cause displacement without surgical stabilization over time.
- Post-traumatic arthritis is the most serious long-term complication and develops when the ankle joint is not perfectly realigned during surgery.
- A bimalleolar fracture with ankle dislocation is a surgical emergency requiring immediate reduction to protect surrounding nerves and blood vessels.
- Full recovery from bimalleolar fracture surgery typically takes 3 to 6 months, with physiotherapy being essential throughout every stage.
- A trimalleolar fracture involves three broken ankle bones instead of two and carries higher complication risk with longer recovery of 4 to 8 months.
- Smoking, diabetes, and poor nutrition significantly slow bimalleolar fracture healing and increase the risk of nonunion and wound complications after surgery.
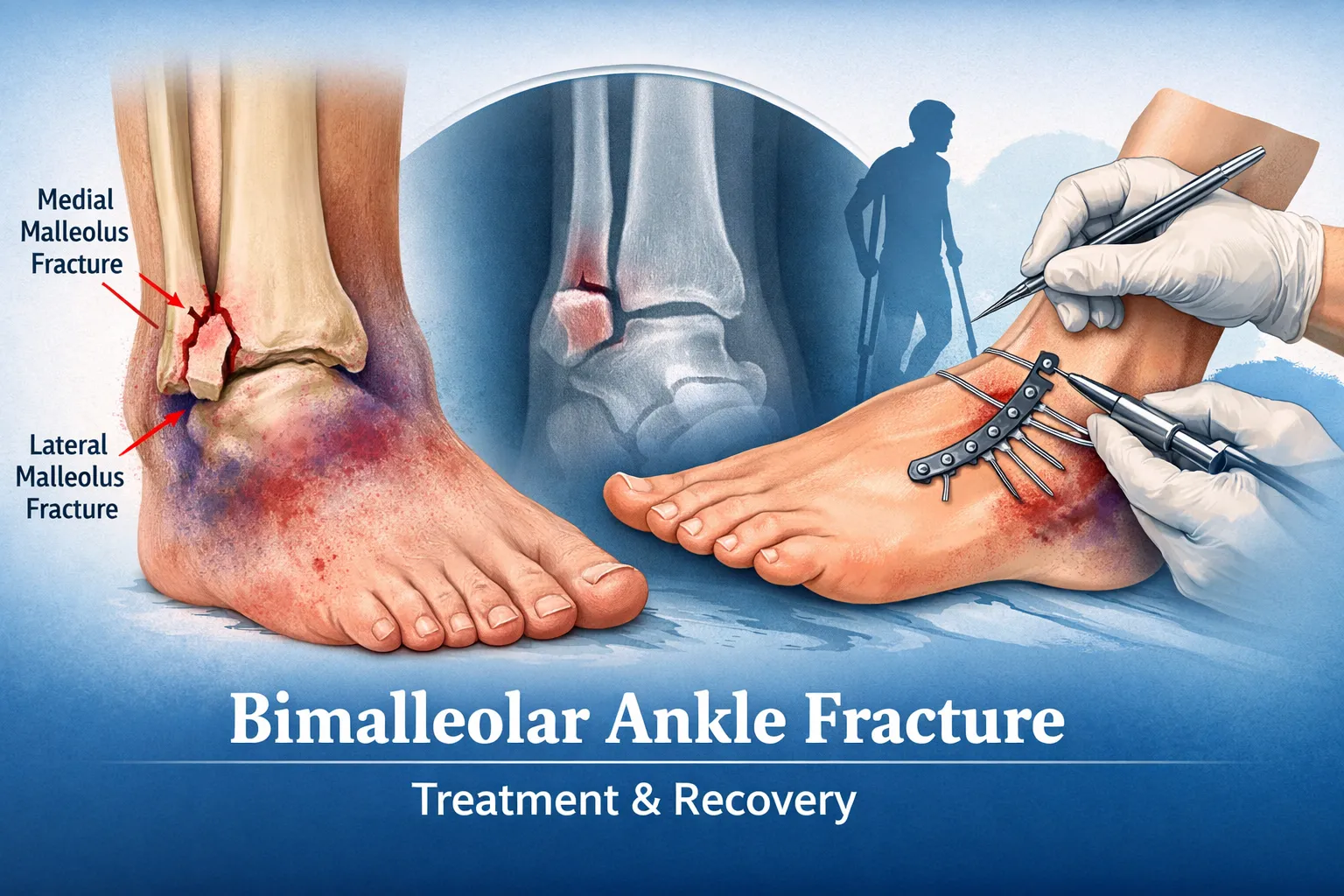
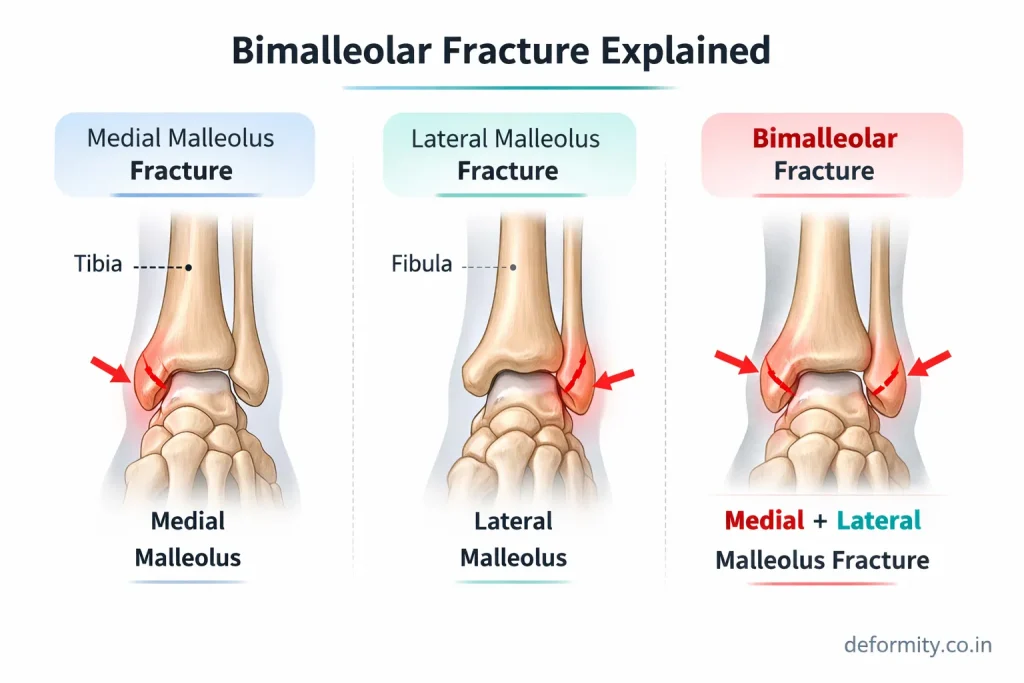
A bimalleolar ankle fracture is a serious injury in which both sides of the ankle joint break – the medial malleolus (inner ankle) and lateral malleolus (outer ankle). Because two stabilizing bones are fractured, the ankle joint becomes unstable and usually requires surgical fixation to restore proper alignment and prevent long-term complications such as arthritis, stiffness, or chronic instability.
This comprehensive guide explains everything about bimalleolar fractures – causes, symptoms, imaging, surgery, fixation methods, recovery timeline, and global treatment options. The article is written for both patients and medical readers and optimized for international search visibility.
Table of Contents
What is a Bimalleolar Fracture?
A bimalleolar fracture refers to a break in both malleoli of the ankle:
- Medial malleolus (distal tibia)
- Lateral malleolus (distal fibula)
These two bones form the ankle mortise, which stabilizes the talus and allows smooth movement during walking. When both sides fracture, the ankle joint becomes unstable and cannot properly support body weight.
Key characteristics:
- Involves both inner and outer ankle bones
- Often associated with ligament injury
- Frequently requires surgical fixation
- May occur with ankle dislocation
Because the ankle loses structural stability, early orthopedic evaluation and proper treatment are essential.
Other Names for a Bimalleolar Fracture
Many patients and medical professionals use different terms when referring to this injury. Understanding these names helps when reading reports, searching for information, or discussing the injury with your surgeon.
A bimalleolar fracture is also known as:
- Bi malleolar fracture – a common alternate spelling
- Bimaleolar fracture – phonetic variation used in some regions
- Bimal fracture – a shortened clinical term
- Bi-malleolar fracture – hyphenated form used in medical coding
- Double malleolus fracture – descriptive term referring to both malleoli
- Both malleoli fracture – plain-language equivalent
- ICD-10 code S82.841 – the medical billing code for closed bimalleolar fracture of the right ankle (S82.842 for left)
The word “bimalleolar” comes from the Latin prefix bi (meaning two) and malleolus (meaning small hammer, referring to the bony projections of the ankle). So a bimalleolar fracture literally means a fracture of both small-hammer-shaped bones of the ankle.
When you see terms like bimalleolar fracture, biomolecular fracture, or bimanual fracture in search queries, these are common misspellings of bimalleolar fracture and refer to the same injury.
Anatomy of the Ankle in Bimalleolar Fracture
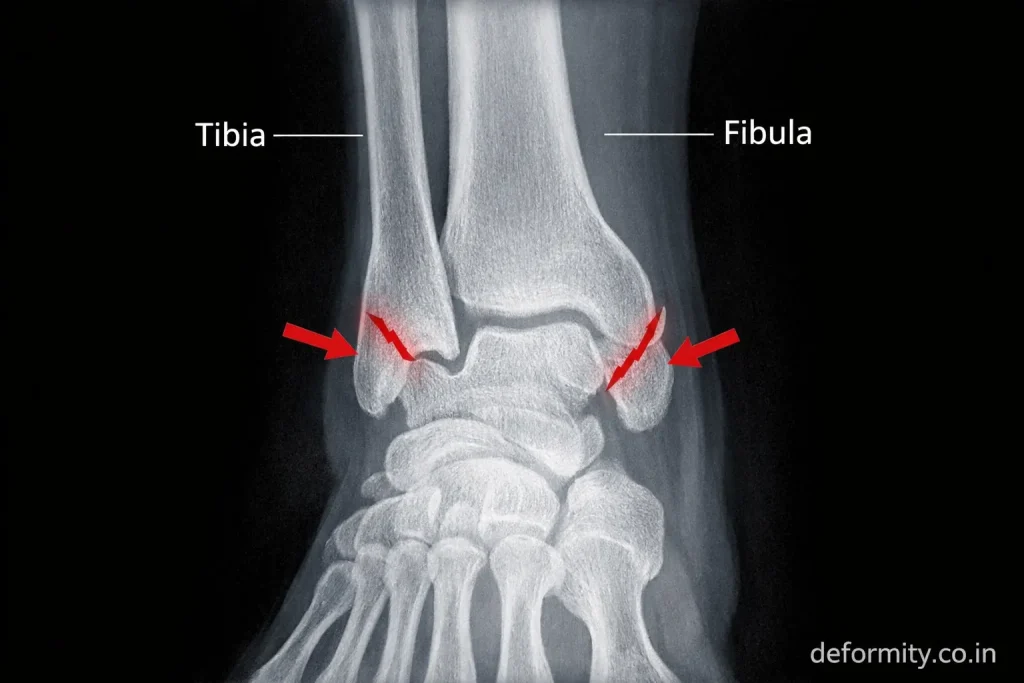
The ankle joint consists of:
- Tibia
- Fibula
- Talus
- Medial malleolus
- Lateral malleolus
Together, these structures form a stable socket that supports body weight. Ligaments surrounding the ankle – particularly the deltoid ligament and syndesmotic ligaments – help maintain alignment.
In a bimalleolar fracture:
- Both stabilizing bones are broken
- Joint alignment is disrupted
- Ligaments may be injured
- Weight-bearing becomes difficult or impossible
Without proper fixation, the talus can shift, leading to long-term joint damage.
The Role of the Fibula and Lateral Malleolus
The fibula is the slender bone that runs parallel to the tibia on the outer side of the lower leg. At its lower end, it forms the lateral malleolus – the bony bump you can feel on the outside of your ankle.
The lateral malleolus plays a critical role in ankle stability. It forms the outer wall of the ankle mortise and prevents the talus from shifting outward. When the lateral malleolus fractures alongside the medial malleolus, both walls of this mortise are compromised, which is why bimalleolar fractures are so mechanically unstable.
Where exactly is the bimalleolar fracture located?
- The medial malleolus fracture occurs at the inner ankle, at the lower end of the tibia, typically just above the ankle joint line
- The lateral malleolus fracture occurs at the outer ankle, at the lower end of the fibula, usually at or just above the level of the ankle joint
The precise level of the fibula fracture determines the fracture classification and influences treatment planning.
Causes of Bimalleolar Ankle Fracture
Bimalleolar fractures typically result from high-energy trauma or severe twisting injuries.
Common causes include:
- Road traffic accidents
- Sports injuries
- Severe ankle twisting
- Falls from height
- Slip and fall accidents
- Osteoporosis-related fractures
Athletes, accident victims, and elderly individuals are at higher risk. In older adults, even minor falls may cause bimalleolar fractures due to reduced bone density.
Mechanism of Injury
Most bimalleolar fractures occur due to rotational forces applied to the ankle.
Typical mechanisms:
- External rotation of the foot
- Supination injury
- Pronation injury
- Twisting with planted foot
These forces can break both malleoli and sometimes damage ligaments. Classification systems like Weber and Lauge-Hansen help determine fracture pattern and stability.
Classification of Bimalleolar Fracture
Proper classification of a bimalleolar fracture is essential because it guides the choice of treatment, the surgical approach, and the expected recovery.
Weber Classification (Based on Fibula Fracture Level)
The Danis-Weber classification is the most widely used system for ankle fractures. It categorizes fractures based on where the fibula breaks in relation to the ankle joint (syndesmosis).
- Weber A – Fibula fractures below the syndesmosis. The ankle joint is usually stable. Often treated without surgery.
- Weber B – Fibula fractures at the level of the syndesmosis. Stability depends on ligament integrity. May or may not require surgery.
- Weber C – Fibula fractures above the syndesmosis. The ankle is almost always unstable. Surgery is typically required.
In bimalleolar fractures, Weber B and C are the most common patterns, and both usually require surgical fixation.
Lauge-Hansen Classification (Based on Injury Mechanism)
The Lauge-Hansen system classifies ankle fractures according to foot position and the direction of force at the time of injury:
- Supination-Adduction (SA)
- Supination-External Rotation (SER) – the most common mechanism for bimalleolar fractures
- Pronation-Abduction (PA)
- Pronation-External Rotation (PER)
This classification helps surgeons understand which ligaments are likely injured and how the fracture pattern should be fixed.
Displaced vs Non-Displaced Bimalleolar Fracture
One of the most important distinctions in bimalleolar fracture management is whether the fracture is displaced or non-displaced, and whether it is open or closed.
Displaced Bimalleolar Fracture
A displaced bimalleolar fracture means the broken bone fragments have shifted out of their normal alignment.
Key features:
- The bone ends are no longer properly aligned
- The ankle mortise is disrupted
- The talus may shift (talar shift)
- The ankle is unstable
- Surgery is almost always required
Displaced fractures are more complex to treat and carry a higher risk of complications such as arthritis and chronic instability if not properly fixed.
Non-Displaced Bimalleolar Fracture
A non-displaced (or nondisplaced) bimalleolar fracture means both malleoli are broken, but the bone fragments remain in their correct position.
Key features:
- Bone fragments are still properly aligned
- The ankle mortise may still be intact
- May be treated conservatively in selected cases
- Requires close monitoring as displacement can still occur
Even non-displaced bimalleolar fractures must be carefully evaluated, because the underlying instability can cause the fracture to displace over time without surgical stabilization.
Closed vs Open Bimalleolar Fracture
- Closed bimalleolar fracture – the skin is intact over the fracture site. This is the most common presentation. Coded as S82.841 (right ankle) or S82.842 (left ankle) in ICD-10.
- Open bimalleolar fracture – a bone fragment has pierced through the skin, creating a wound. This is a surgical emergency because of the risk of infection. Open fractures require urgent washout and fixation.
Most bimalleolar fractures encountered in clinical practice are closed fractures, but open fractures require faster intervention.
Bimalleolar Equivalent Fracture: What It Means
A bimalleolar equivalent fracture is a term that confuses many patients and even some clinicians. It is important to understand.
In a true bimalleolar fracture, both the medial malleolus (bone) and the lateral malleolus (bone) are fractured.
In a bimalleolar equivalent fracture:
- The lateral malleolus (fibula) is fractured
- But instead of the medial malleolus bone breaking, the deltoid ligament tears completely
Because the deltoid ligament provides the same medial stability as the medial malleolus bone, its complete rupture creates the same degree of ankle instability as a true bimalleolar fracture.
In functional terms, a bimalleolar equivalent fracture behaves exactly like a bimalleolar fracture – the ankle joint is unstable and usually requires surgical treatment.
Why does this matter?
On initial X-ray, a bimalleolar equivalent fracture may look like a simple lateral malleolus fracture. The medial side appears intact because the ligament (not the bone) is what has failed. This can lead to underdiagnosis if the medial instability is not carefully assessed with stress imaging or MRI.
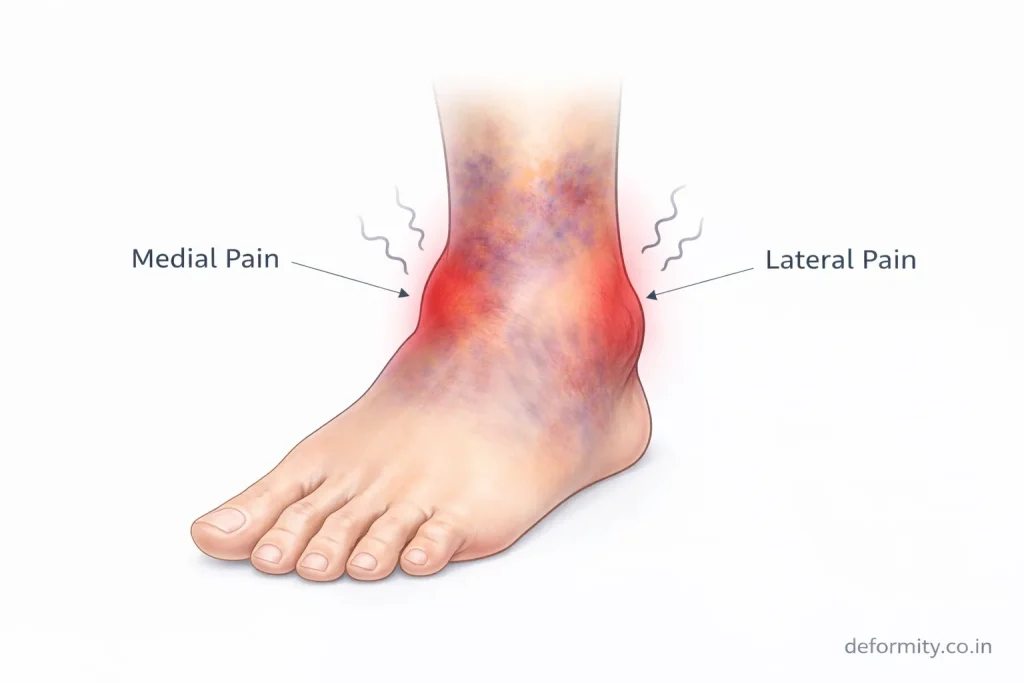
Any lateral malleolus fracture with medial tenderness, bruising over the inner ankle, or widening of the medial clear space on X-ray should be evaluated for a bimalleolar equivalent injury.
Bimalleolar Fracture with Ankle Dislocation
In severe injuries, a bimalleolar fracture can occur alongside complete ankle dislocation – a condition where the talus is forced entirely out of the ankle mortise.
This is known as a fracture-dislocation of the ankle and is a surgical emergency.
Key features:
- The ankle appears grossly deformed
- The talus is displaced from its normal position
- Skin may be under tension (at risk of breaking down)
- Blood vessel and nerve injury is possible
- Requires immediate reduction (repositioning) before surgery
Emergency treatment involves:
- Urgent closed reduction – gently repositioning the ankle without surgery to relieve pressure on the skin and neurovascular structures
- Temporary splinting to hold the reduced position
- Early surgical fixation once swelling is controlled
Bimalleolar fracture-dislocations have a higher complication rate than simple bimalleolar fractures and require prompt specialist intervention to protect the joint and surrounding soft tissues.
Symptoms of Bimalleolar Fracture
Symptoms are usually severe and immediate.
Common signs include:
- Severe ankle pain
- Swelling
- Bruising
- Visible deformity
- Inability to bear weight
- Reduced ankle movement
In some cases, the ankle may appear misaligned or dislocated. Because this injury affects joint stability, walking is usually not possible.
Diagnosis
Early diagnosis is critical to prevent complications.
Physical Examination
An orthopedic specialist evaluates:
- Swelling
- Bone tenderness
- Deformity
- Stability
- Neurovascular status
X-ray Imaging
X-rays confirm the diagnosis and show the fracture pattern.
Standard views:
- AP view
- Lateral view
- Mortise view
These help determine displacement and joint alignment.
CT Scan
A CT scan may be required when:
- Fracture pattern is complex
- Posterior malleolus involved
- Surgical planning needed
Advanced imaging helps assess joint congruity and fixation requirements.
Is a Bimalleolar Fracture Stable?
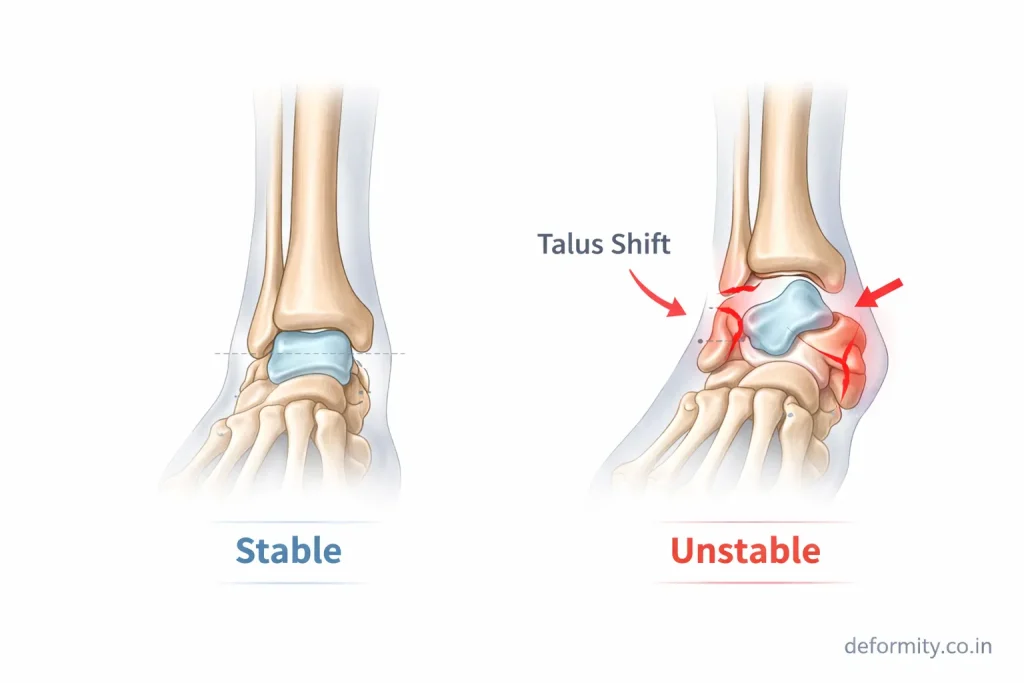
A bimalleolar fracture is almost always unstable because both sides of the ankle joint are broken.
Features of instability:
- Joint misalignment
- Ligament injury
- Talar shift
- Inability to bear weight
Because of this instability, most cases require surgical fixation to restore proper alignment and allow healing.
Treatment of Bimalleolar Fracture
Treatment depends on fracture displacement, patient health, and associated injuries.
Emergency Management
Initial treatment includes:
- Splint immobilization
- Elevation
- Ice therapy
- Pain management
- Urgent orthopedic evaluation
In cases of severe swelling or dislocation, temporary reduction may be required before surgery.
Surgical Treatment (ORIF)
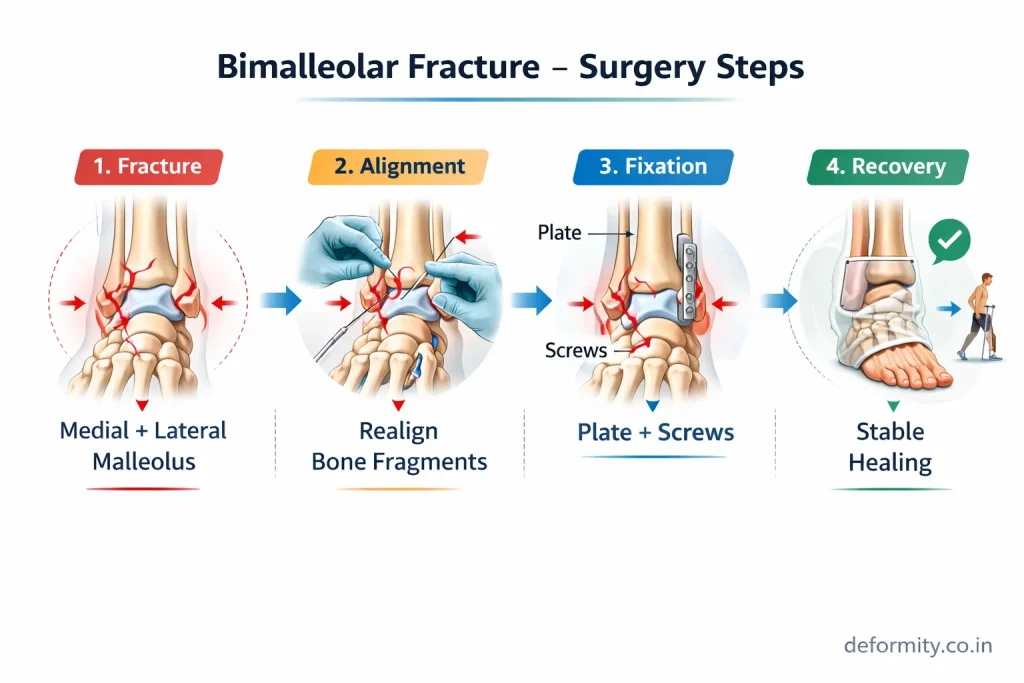
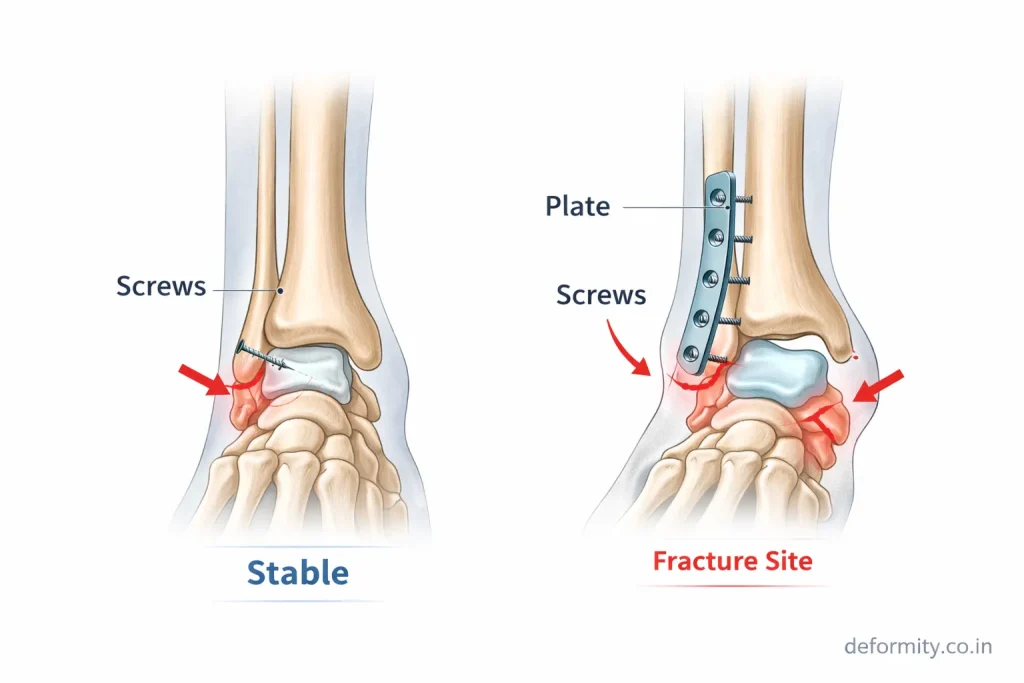
Most bimalleolar fractures require Open Reduction and Internal Fixation (ORIF).
The procedure involves:
- Realigning bone fragments
- Fixing the medial malleolus with screws
- Fixing the lateral malleolus with a plate and screws
- Stabilizing the syndesmosis if needed
Goals of surgery:
- Restore joint alignment
- Maintain ankle stability
- Prevent arthritis
- Enable early rehabilitation
Dr Divya Ahuja uses advanced fixation techniques to achieve anatomical alignment and faster functional recovery.
Non-Surgical Treatment (Rare)
Non-surgical treatment may be considered when:
- Fracture not displaced
- Patient is medically unfit for surgery
- Low functional demand
Management includes casting and strict immobilization, but outcomes are generally better with surgical fixation.
Recovery Time After Bimalleolar Fracture
Recovery varies depending on severity and treatment.
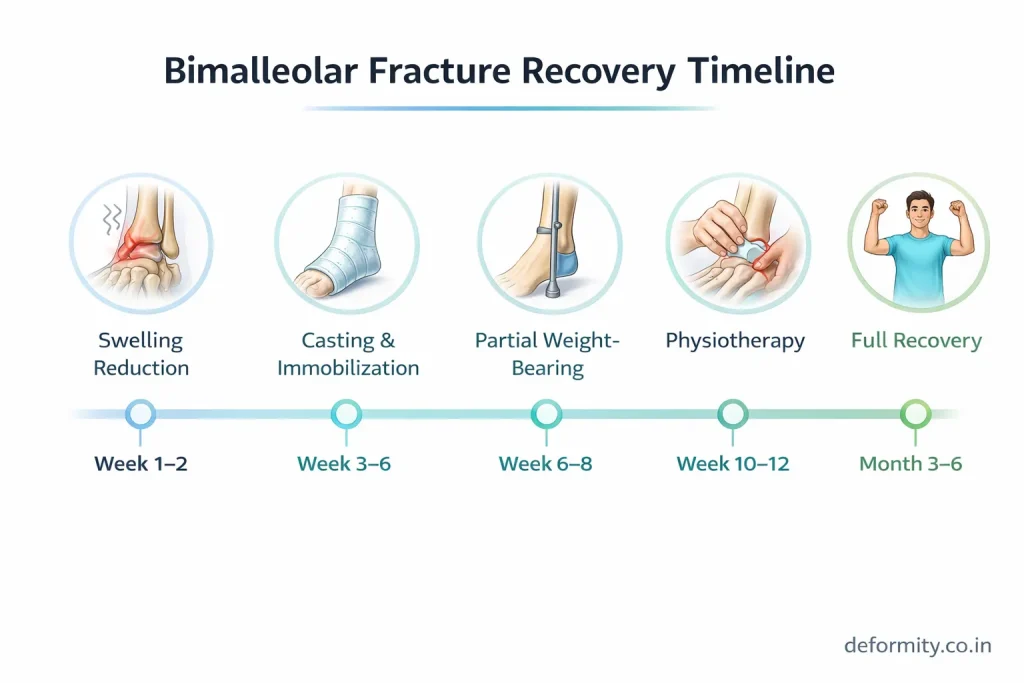
| Phase | Timeline |
|---|---|
| Immobilization | 6 weeks |
| Partial weight-bearing | 6–8 weeks |
| Walking without support | 10–12 weeks |
| Full recovery | 3–6 months |
Recovery stages include:
- Swelling reduction
- Bone healing
- Physiotherapy
- Strength rebuilding
- Return to activity
Most patients regain good mobility with proper rehabilitation.
Factors That Affect Recovery Time
Several factors can extend or shorten the standard recovery timeline:
Factors that slow recovery:
- Older age and reduced bone density
- Displaced or comminuted fractures
- Associated ligament injury or dislocation
- Diabetes, peripheral vascular disease, or smoking
- Delayed surgery or inadequate fixation
- Poor compliance with physiotherapy
Factors that support faster recovery:
- Younger age and healthy bone quality
- Non-displaced or minimally displaced fracture
- Early surgical fixation with stable construct
- Dedicated physiotherapy programme
- Good nutrition including adequate calcium and vitamin D
- No associated medical comorbidities
The bimalleolar ankle fracture surgery recovery time can also vary depending on which ankle is involved. A right bimalleolar fracture may temporarily affect driving ability, while a left bimalleolar fracture may impact gait and balance during recovery. Neither side heals faster than the other – the timeline is determined by the fracture complexity, not the side.
Rehabilitation & Physiotherapy
Rehabilitation is essential for restoring function.
Key components:
- Range of motion exercises
- Strength training
- Balance exercises
- Gait training
- Functional movement training
Skipping physiotherapy can result in stiffness and weakness.
ORIF Rehabilitation Protocol After Bimalleolar Fracture
After ORIF surgery for a bimalleolar fracture, rehabilitation follows a structured, stage-based protocol. The exact timeline is set by the treating surgeon based on fixation stability and healing progress, but the general framework is as follows:
Phase 1 – Protection and Swelling Control (Weeks 0–2)
- Non-weight-bearing with crutches
- Limb elevation to reduce swelling
- Gentle toe and knee exercises to maintain circulation
- Wound care and monitoring for infection
Phase 2 – Early Mobilization (Weeks 2–6)
- Ankle range of motion exercises begin (dorsiflexion, plantarflexion, inversion, eversion)
- Non-weight-bearing maintained until bone healing confirmed on X-ray
- Gentle strengthening of hip and knee muscles to prevent deconditioning
- Pool therapy may begin if wound is fully healed
Phase 3 – Progressive Weight-Bearing (Weeks 6–10)
- Gradual progression from toe-touch to partial to full weight-bearing
- Walking boot or cast may be used during this phase
- Strengthening exercises for the calf, peroneal muscles, and tibialis anterior
- Balance and proprioception training begins
Phase 4 – Functional Recovery (Weeks 10–16+)
- Full weight-bearing walking without support
- Return to stairs, slopes, and uneven ground
- Sport-specific training for athletes
- Gradual return to recreational and occupational activities
Phase 5 – Return to Sport / Full Activity (Months 4–6)
- Functional testing to confirm strength and balance symmetry
- Clearance for running, jumping, and pivoting activities
- Long-term ankle strengthening to prevent re-injury
Adherence to the physiotherapy programme is one of the strongest predictors of long-term ankle function after bimalleolar fracture ORIF.
Complications
If not treated properly, complications may occur.
Possible complications include:
- Post-traumatic arthritis
- Malunion
- Nonunion
- Infection
- Chronic stiffness
- Hardware irritation
Early surgery and rehabilitation reduce these risks significantly.
Understanding Bimalleolar Fracture Complications in Detail
Each complication carries its own implications for long-term outcome:
Post-traumatic arthritis is the most common long-term complication. When the cartilage surface of the ankle joint is damaged at the time of injury – or if the joint is not perfectly realigned – early arthritis can develop within 5–10 years. Precise anatomical reduction during surgery is the primary protection against this outcome.
Malunion occurs when the bone heals in an abnormal position. This is more likely with non-surgical treatment or if fixation is inadequate. Malunion causes abnormal load distribution across the ankle joint, accelerating wear and causing pain with walking.
Nonunion means the bone fragments fail to heal together. This is less common in the ankle than in other fractures but can occur in smokers, diabetics, or patients with poor blood supply.
Wound infection and hardware complications are surgical risks. Deep infection requires antibiotic treatment and sometimes additional surgery. Hardware (plates and screws) may occasionally cause irritation through the skin and can be removed after the fracture is fully healed, typically after 12–18 months.
Chronic ankle instability can result if ligament injuries associated with the fracture are not addressed. Persistent ligament laxity causes the ankle to feel unstable during walking and sporting activity.Stiffness is common after prolonged immobilization and is addressed through dedicated physiotherapy. Early mobilization after surgery significantly reduces the degree of residual stiffness.
Right vs Left Bimalleolar Fracture
Both right and left bimalleolar fractures require similar treatment, but daily activities may differ.
A right ankle fracture may affect:
- Driving
- Work requiring pedals
Left ankle fracture may affect:
- Walking balance
- Weight-bearing
The recovery timeline is similar for both sides.
Bimalleolar vs Trimalleolar Fracture
A trimalleolar fracture involves an additional posterior malleolus fracture and is more complex.
Comparison:
- Bimalleolar → two bones fractured
- Trimalleolar → three bones fractured
- Trimalleolar injuries are often more severe
Internal linking between pages improves SEO authority.
Trimalleolar Fracture: Deeper Comparison
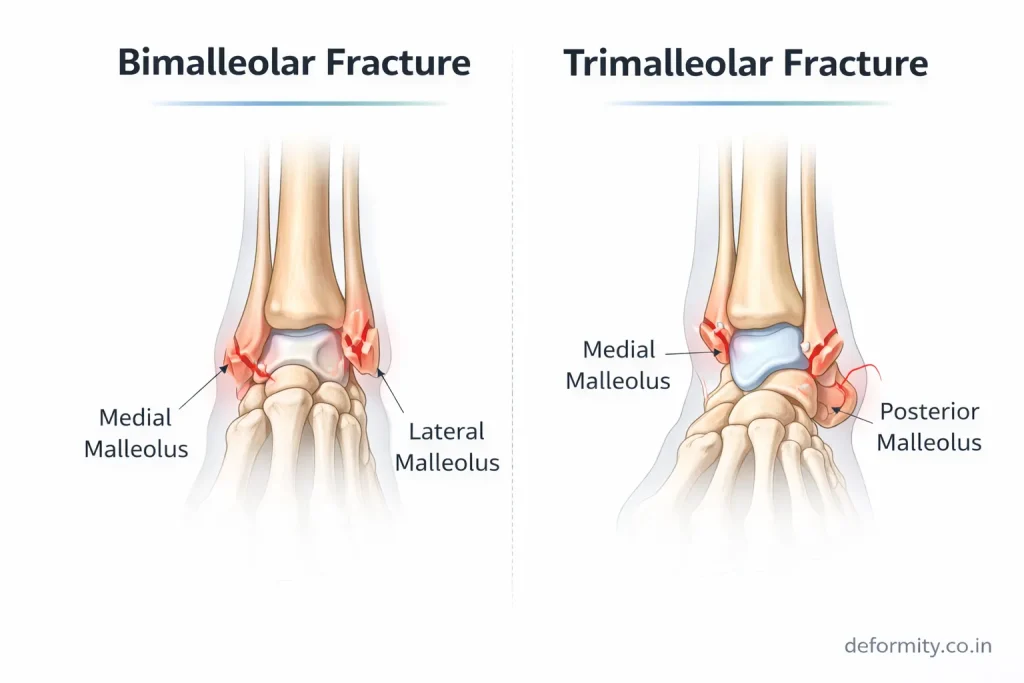
A trimalleolar fracture – also known as a Cotton fracture – is considered one of the most complex ankle fractures. It involves the medial malleolus, lateral malleolus, and the posterior malleolus (the back portion of the tibia that forms the rear wall of the ankle joint).
Key differences between bimalleolar and trimalleolar fractures:
| Feature | Bimalleolar Fracture | Trimalleolar Fracture |
| Bones involved | 2 (medial + lateral malleolus) | 3 (medial + lateral + posterior malleolus) |
| Joint stability | Severely compromised | Maximally compromised |
| Surgery required | Almost always | Always |
| Posterior fixation needed | No | Yes, if fragment >25% of joint surface |
| Recovery time | 3–6 months | 4–8 months |
| Complication risk | Moderate | Higher |
| Also known as | Bi malleolar fracture | Cotton fracture, tri-malleolar fracture |
Trimalleolar fracture treatment always involves surgical fixation of the lateral and medial malleoli. The posterior malleolus is fixed if the fragment is large enough to destabilize the joint – generally when it involves more than 25% of the tibial articular surface.
Trimalleolar fracture recovery time is longer than for a bimalleolar fracture. Most patients begin weight-bearing between 8–10 weeks and achieve full recovery between 4–8 months, depending on the complexity of the injury and the quality of fixation. Rehabilitation follows a similar phased protocol to bimalleolar fractures but progresses more gradually.
When to See an Orthopedic Specialist
Seek urgent care if:
- Severe ankle pain
- Visible deformity
- Cannot bear weight
- Swelling increasing
- Injury after a fall or accident
Early treatment improves outcomes and reduces long-term complications.
Treatment in India & International Consultation
Many global patients choose India for ankle fracture surgery due to advanced orthopedic care and cost advantages.
Dr Divya Ahuja provides specialized treatment for:
- Bimalleolar fractures
- Complex ankle injuries
- Revision surgeries
- Sports trauma
International patients can access:
- Online consultation
- Treatment planning
- Affordable surgery
- Rehabilitation guidance
Early expert treatment ensures proper healing and long-term ankle stability.
Conclusion
A bimalleolar ankle fracture is a serious injury that affects joint stability and mobility. Proper diagnosis, timely surgical fixation, and structured rehabilitation are essential for full recovery. With modern orthopedic techniques and physiotherapy, most patients regain good function and return to daily activities without long-term problems.
Explore all our fracture-related blogs
| Topic | Link |
| Cervical Radiculopathy | Click here |
| Distal Radius Fracture | Click here |
| Proximal Humerus Fracture | Click here |
| Lauge-Hansen Classification of Ankle Fractures | Click here |
| Weber Classification of Ankle Fractures | Click here |
| Trimalleolar Fracture | Click here |
| Bimalleolar Ankle Fracture | Click here |
| Lateral Malleolus Fracture | Click here |
| Medial Malleolus Fracture | Click here |
| Complete Guide to Ankle Fractures | Click here |
| Femur Shaft Fractures | Click here |
| Tibia Fracture | Click here |
FAQs
How long does a bimalleolar fracture take to heal?
Most bimalleolar fractures heal in 6–8 weeks, but full recovery, including strength and mobility, may take 3–6 months, depending on surgery and rehabilitation.
Does a bimalleolar fracture always need surgery?
Most cases require surgery because the ankle becomes unstable when both malleoli are fractured. Stable, non-displaced fractures may occasionally be treated conservatively.
Can you walk after bimalleolar fracture surgery?
Walking usually begins gradually after 6–8 weeks once bone healing is confirmed. Full weight-bearing depends on the surgeon’s advice and recovery progress.
What is bimalleolar fracture fixation?
Fixation involves surgically aligning the broken bones and stabilizing them using plates and screws. This restores joint alignment and allows proper healing.
Is a bimalleolar fracture serious?
Yes. Because both sides of the ankle are broken, the joint becomes unstable and requires proper treatment to prevent long-term complications.
What is a bimalleolar equivalent fracture?
A bimalleolar equivalent fracture involves a lateral malleolus fracture combined with complete rupture of the deltoid ligament instead of a medial malleolus bone fracture. It creates the same ankle instability as a true bimalleolar fracture and is treated similarly.
What is the difference between a bimalleolar and trimalleolar fracture?
A bimalleolar fracture breaks two bones (medial and lateral malleolus). A trimalleolar fracture, also known as a Cotton fracture, breaks three bones – the same two plus the posterior malleolus. Trimalleolar fractures are more severe and take longer to recover.
What is a displaced bimalleolar fracture?
A displaced bimalleolar fracture means the broken bone fragments have shifted out of alignment. This almost always requires surgery to restore joint congruity and prevent long-term complications like arthritis.
What is a closed bimalleolar fracture?
A closed bimalleolar fracture means the skin over the fracture site is intact. This is the most common type and is coded as S82.841 (right ankle) or S82.842 (left ankle) in medical records.