A trimalleolar fracture is a severe ankle injury involving three components of the ankle joint – the medial malleolus, lateral malleolus, and posterior malleolus. Because all major stabilizing structures are disrupted, this injury is highly unstable and almost always requires surgical fixation to restore alignment and prevent long-term complications such as arthritis, stiffness, or chronic pain.
This comprehensive guide provides in-depth explanations of trimalleolar ankle fractures, including anatomy, radiological findings, surgical techniques, fixation methods, recovery timelines, and long-term outcomes. The content is designed for patients, caregivers, medical learners, and international readers seeking expert treatment options.
Table of Contents
What is a Trimalleolar Fracture?

A trimalleolar fracture occurs when three bony structures of the ankle joint break simultaneously:
- Medial malleolus (inner ankle – tibia)
- Lateral malleolus (outer ankle – fibula)
- Posterior malleolus (back part of the distal tibia)
This injury affects the entire ankle mortise, the socket that holds the talus in place. When all three malleoli are fractured, the ankle joint becomes unstable, often accompanied by ligament injury and sometimes ankle dislocation.
Key characteristics:
- Involves three fracture components
- Highly unstable injury
- Frequently associated with ligament damage
- Almost always requires surgery
Because the posterior malleolus is involved, joint surface integrity is compromised, increasing the risk of arthritis if not properly treated.
Anatomy of the Ankle in Trimalleolar Fracture
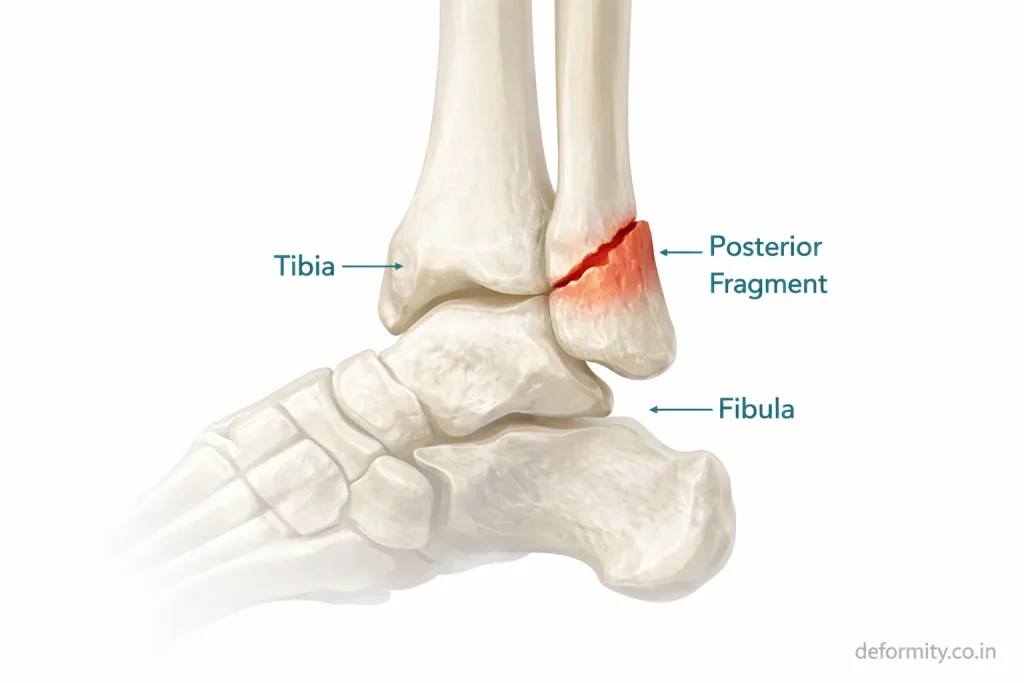
The ankle joint consists of:
- Tibia
- Fibula
- Talus
- Medial malleolus
- Lateral malleolus
- Posterior malleolus
Together, these form the ankle mortise – a stable socket that supports body weight and allows motion.
In trimalleolar fractures:
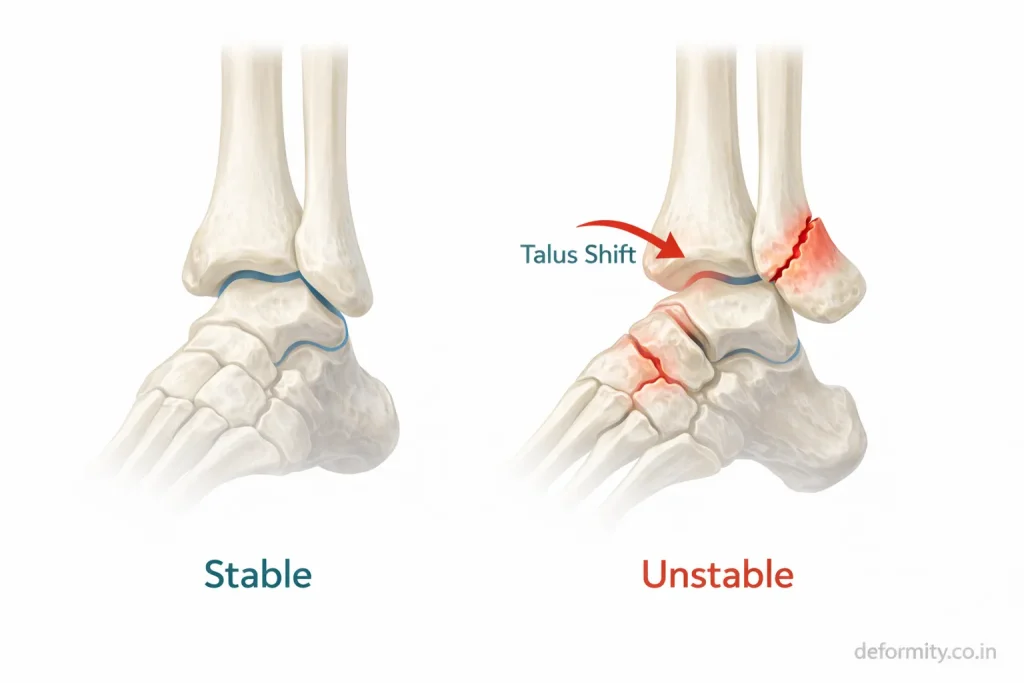
- Both sides of the ankle break
- The posterior tibial fragment detaches
- Syndesmotic ligaments may be injured
- The talus may shift out of alignment
Because all structural supports are compromised, joint congruity must be restored surgically.
Why the Posterior Malleolus Matters
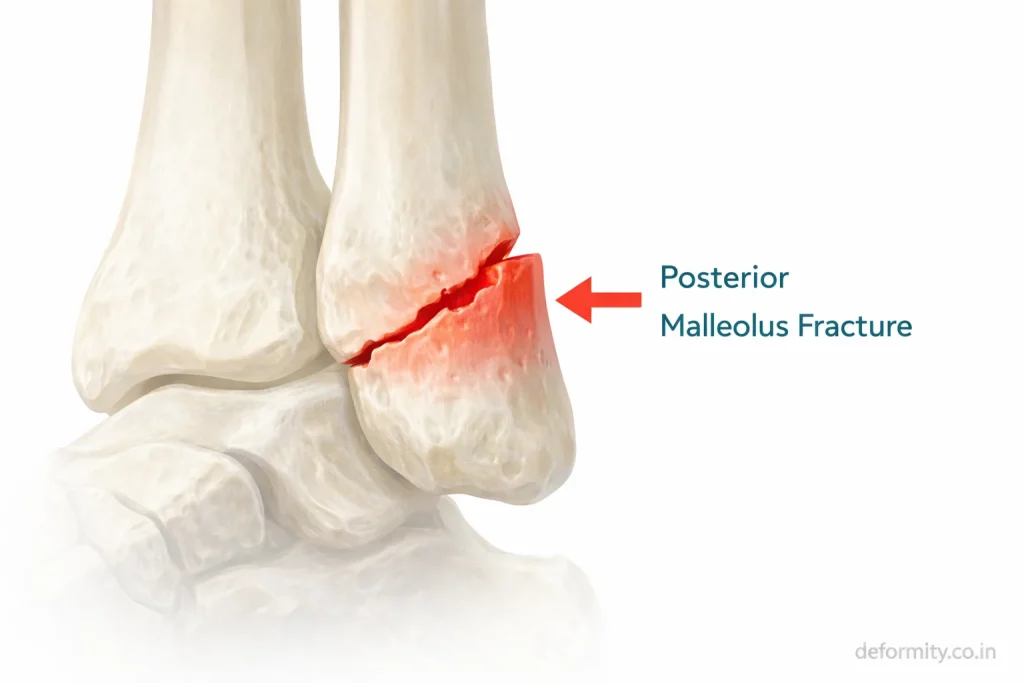
The posterior malleolus is the back portion of the distal tibia. It forms part of the weight-bearing surface of the ankle joint and provides attachment to the posterior inferior tibiofibular ligament.
Its importance includes:
- Maintaining ankle stability
- Supporting the joint surface
- Preserving syndesmotic integrity
- Preventing talar displacement
When the posterior fragment involves more than 25–30% of the joint surface, surgical fixation is strongly recommended to restore alignment and reduce the risk of arthritis.
Causes of Trimalleolar Ankle Fracture
Trimalleolar fractures usually result from high-energy trauma or severe rotational forces.
Common causes include:
- Road traffic accidents
- Fall from height
- Severe ankle twisting
- Sports trauma
- High-impact injuries
- Osteoporotic fractures in the elderly
Young individuals typically sustain these injuries in accidents, while older adults may suffer them after falls due to bone fragility.
Mechanism of Injury
Most trimalleolar fractures occur due to rotational forces applied to the ankle.
Typical mechanisms:
- Supination-external rotation injury
- Pronation injury
- Twisting with planted foot
- High rotational trauma
Classification systems such as Weber and Lauge-Hansen help describe fracture patterns and guide surgical planning.
Trimalleolar Fracture Classification
Understanding how a trimalleolar fracture is classified helps explain the surgical approach chosen and influences recovery expectations.
Weber Classification is based on the level of the lateral malleolus fracture:
- Weber A – Fracture below the syndesmosis; usually stable
- Weber B – Fracture at the level of the syndesmosis; may be unstable
- Weber C – Fracture above the syndesmosis; syndesmotic injury likely
In trimalleolar fractures, Weber B and C patterns are most common.
Lauge-Hansen Classification describes the mechanism of injury:
- Supination-Adduction (SA)
- Supination-External Rotation (SER) – most common pattern in trimalleolar fractures
- Pronation-Abduction (PA)
- Pronation-External Rotation (PER)
The Lauge-Hansen classification helps surgeons predict which structures are injured even before imaging and plan the order of fixation during surgery.
Symptoms of Trimalleolar Fracture

Symptoms are typically severe and immediate.
Common signs include:
- Intense ankle pain
- Rapid swelling
- Bruising
- Visible deformity
- Inability to bear weight
- Restricted movement
Because the joint is unstable, walking is usually impossible without medical support.
How Painful is a Trimalleolar Fracture?
A trimalleolar fracture is considered one of the most painful ankle injuries. The pain arises from multiple fracture sites simultaneously, combined with significant soft tissue swelling and, in some cases, joint dislocation.
Patients typically describe:
- Sharp, immediate pain at the time of injury
- Throbbing pain that worsens with any movement
- Pressure-like pain from swelling inside the ankle
- Sensitivity even to light touch around the ankle
Pain management is a priority in the early stages of treatment and is handled with a combination of elevation, immobilisation, ice, and medications prescribed by the treating doctor.
Trimalleolar Fracture Radiology
Radiology plays a critical role in diagnosis and surgical planning.
X-ray Findings
Standard X-ray views include:
- AP view
- Lateral view
- Mortise view
Findings may show:
- Fracture lines on the medial and lateral sides
- Posterior malleolus fragment on lateral view
- Joint misalignment
- Talar shift
Trimalleolar Fracture X-ray: What to Look For
On a trimalleolar fracture X-ray, the key findings that confirm the diagnosis include:
- AP view – fracture lines visible through the medial and lateral malleoli; widening of the medial clear space if there is talar shift
- Lateral view – posterior malleolus fragment visible as a separate piece off the back of the tibia; posterior displacement of the talus may be seen
- Mortise view – disruption of the joint space symmetry; syndesmotic widening if the tibiofibular ligaments are injured
The posterior malleolus fragment is often best appreciated on the lateral X-ray view. However, its true size relative to the joint surface can only be accurately measured on CT scan, which is why X-ray alone is usually insufficient for full surgical planning.
CT Scan Importance
CT scans are often recommended because:
- Posterior fragment size must be measured
- Joint surface congruity must be assessed
- Fragment displacement must be evaluated
- Surgical planning requires precise imaging
CT imaging provides a 3D understanding of fracture geometry and helps determine fixation strategy.
Trimalleolar Fracture CT: Key Findings
A CT scan of a trimalleolar fracture provides critical information that X-rays cannot:
- Exact percentage of the joint surface involved in the posterior fragment
- Number of bone fragments (comminution)
- Degree of displacement of each fracture component
- Articular step-off measurements
- Status of the syndesmosis and surrounding ligaments
CT is considered essential before surgery when the posterior malleolus is involved. It helps the surgeon choose the best fixation approach – whether anteroposterior screw fixation or a posterior plate will give better stability.
On CT, a posterior fragment involving more than 25% of the joint surface is a strong indicator for fixation to prevent talar instability and long-term arthritis.
Radiology Features of Instability
Radiological signs of instability include:
- Syndesmotic widening
- Medial clear space widening
- Talar displacement
- Posterior fragment displacement
Detailed radiological evaluation ensures accurate treatment planning.
Displaced vs Non-Displaced Trimalleolar Fracture
One of the most important distinctions in trimalleolar fracture management is whether the fracture is displaced or non-displaced.
Non-displaced trimalleolar fracture:
- The bone fragments remain in their correct anatomical position
- The joint surface is maintained
- Rare in trimalleolar injuries due to the high-energy mechanism involved
- May occasionally be managed conservatively with close monitoring
- Still requires specialist evaluation and imaging confirmation
Displaced trimalleolar fracture:
- One or more fragments have shifted out of normal position
- Joint alignment is disrupted
- Talar shift may be present
- Surgical fixation is almost always required
- Higher risk of arthritis if not accurately reduced
Most trimalleolar fractures seen in practice are displaced to some degree. Even a small displacement in the posterior malleolus can significantly affect joint stability and long-term outcomes, which is why CT-guided surgical planning is essential.
Open vs Closed Trimalleolar Fracture
A closed trimalleolar fracture means the fractured bones have not broken through the skin. This is the most common presentation. Although the injury is severe internally, the skin remains intact.
An open trimalleolar fracture means one or more bone fragments have pierced through the skin. This is a surgical emergency requiring urgent debridement (cleaning of the wound) and fracture stabilisation to prevent deep infection.
An open trimalleolar fracture carries a significantly higher risk of:
- Infection, including deep bone infection (osteomyelitis)
- Delayed bone healing
- Soft tissue complications
- Longer recovery
A closed trimalleolar fracture of the right ankle or left ankle is far more common than open fractures and carries a better prognosis when treated promptly with appropriate surgery.
Trimalleolar Fracture with Dislocation
In some cases, a trimalleolar fracture is accompanied by ankle dislocation – meaning the talus shifts completely out of the ankle mortise.
A trimalleolar ankle fracture with dislocation is considered a true orthopaedic emergency. The ankle must be reduced (put back into position) as quickly as possible to:
- Restore blood supply to the ankle and foot
- Prevent skin necrosis over the displaced bone
- Reduce pressure on nerves and vessels
- Improve surgical outcomes
After emergency reduction, the limb is temporarily stabilised. Definitive surgical fixation is then planned once swelling is controlled, usually within 5 to 10 days of injury.Recovery from a trimalleolar fracture with dislocation typically takes longer than a standard trimalleolar fracture – often 9 to 15 months for full functional recovery.
Is a Trimalleolar Fracture Always Surgical?
In most cases, yes.
Because three stabilizing structures are involved, trimalleolar fractures are generally unstable and require surgical fixation. Non-surgical treatment may be considered only if:
- Fractures are non-displaced
- Patient is medically unfit for surgery
- Functional demand is very low
However, surgical treatment typically offers better long-term outcomes.
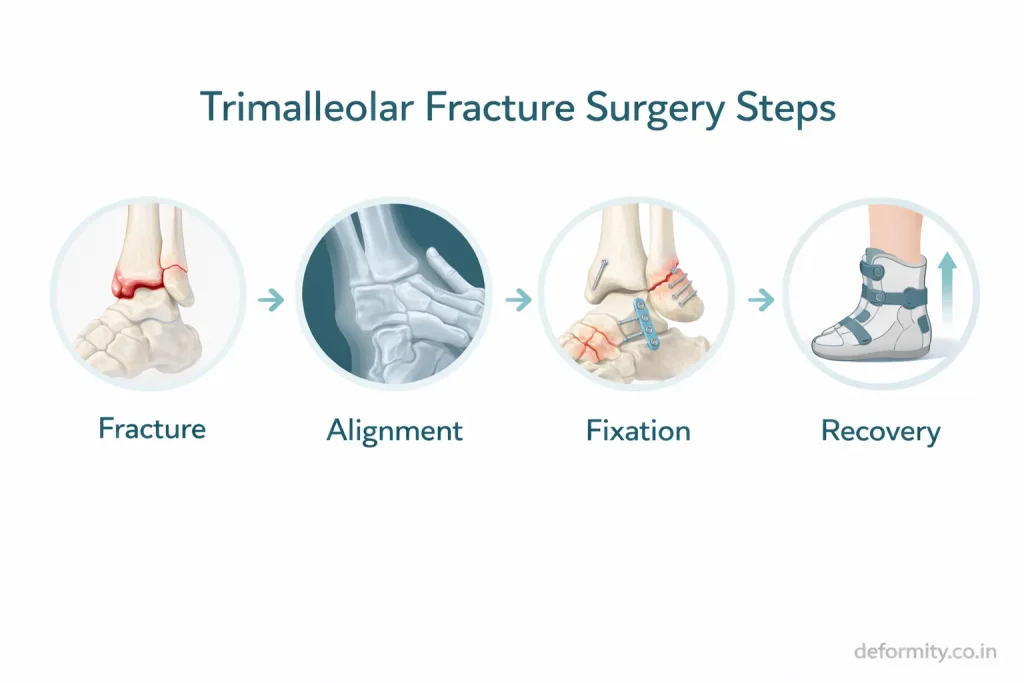
Surgical Treatment of Trimalleolar Fracture
Surgery aims to restore anatomical alignment and joint congruity.
ORIF (Open Reduction and Internal Fixation)
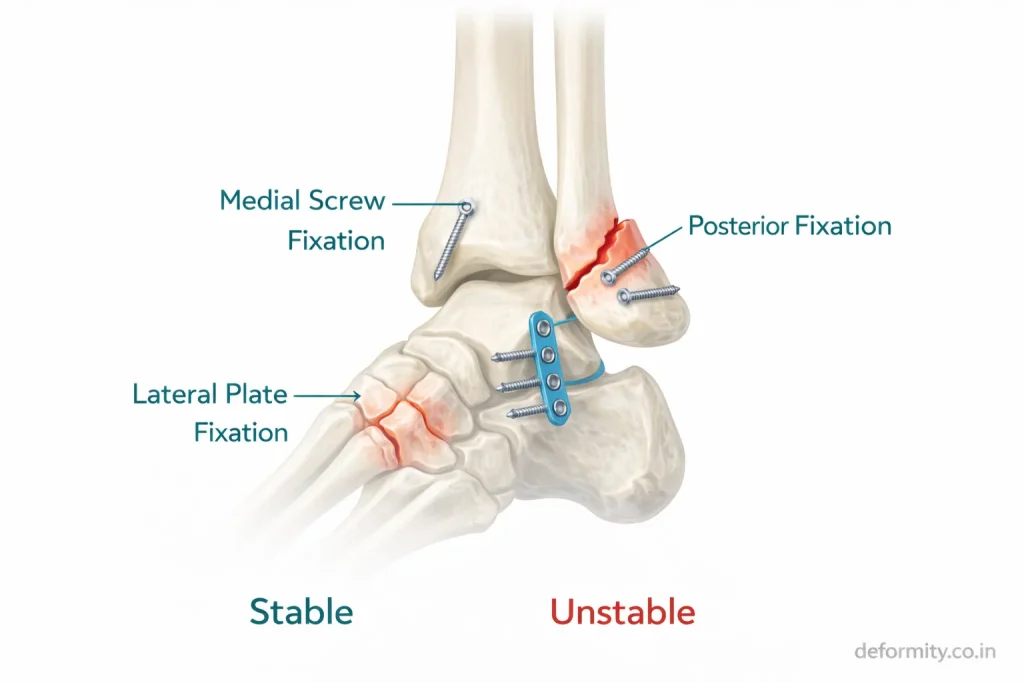
The procedure involves:
- Realigning fracture fragments
- Fixing the medial malleolus with screws
- Fixing the lateral malleolus with a plate and screws
- Fixing the posterior malleolus with screws or a plate
How Long Does Trimalleolar Fracture Surgery Take?
A common patient question is how long the operation lasts.
Trimalleolar fracture surgery (ORIF) typically takes 2 to 4 hours, depending on:
- Complexity and number of fragments
- Whether the syndesmosis needs repair
- Whether an ankle dislocation was present
- Surgical approach chosen for the posterior malleolus
- Patient factors such as swelling and bone quality
Surgeries involving posterior plating or syndesmotic repair tend to take longer than cases requiring only screw fixation. The surgery is performed under spinal or general anaesthesia, and patients are usually admitted for 1 to 3 days postoperatively.
Posterior Malleolus Fixation Techniques
Common approaches include:
- Posterolateral approach
- Anterior-to-posterior screw fixation
- Posterior plating
Proper fixation restores joint stability and prevents talar shift.
Syndesmotic Fixation
If the syndesmotic ligaments are injured:
- Syndesmotic screws
- Tightrope fixation
may be used to maintain alignment during healing.
Dr Divya Ahuja specializes in complex ankle trauma fixation with emphasis on anatomical restoration and early rehabilitation.
External Fixation in Trimalleolar Fracture
In some complex or emergencies, external fixation may be used as a temporary measure before definitive surgery. External fixators hold the bone fragments in position from outside the skin using pins and connecting rods.
External fixation is used when:
- Severe swelling prevents immediate surgery
- Open fractures require wound management first
- Ankle dislocation has compromised skin and soft tissue
- Patient is medically unstable
Once swelling reduces and the soft tissue is in a safer condition, the external fixator is removed and definitive ORIF is performed. This staged approach reduces surgical complications and improves fixation outcomes.
Dr Divya Ahuja specialises in complex ankle trauma fixation with emphasis on anatomical restoration and early rehabilitation.
Recovery After Trimalleolar Fracture
Recovery is longer compared to simpler ankle fractures.
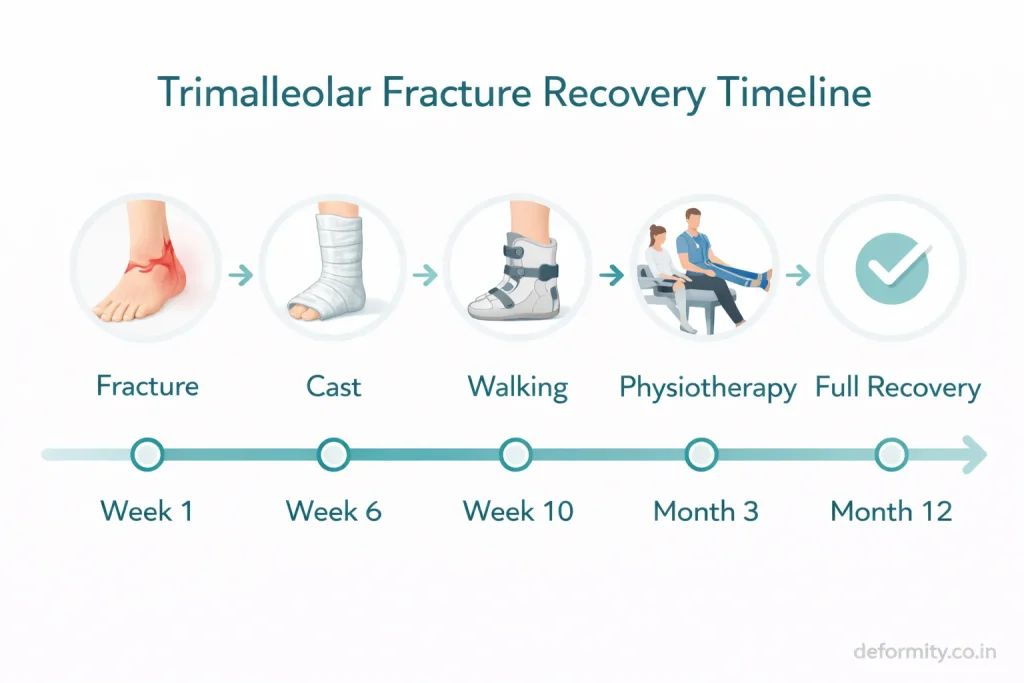
| Stage | Timeline |
|---|---|
| Non-weight bearing | 6 weeks |
| Partial weight-bearing | 8–10 weeks |
| Walking without support | 10–12 weeks |
| Functional recovery | 3–6 months |
| Full recovery | 6–12 months |
Factors influencing recovery:
- Age
- Bone quality
- Rehabilitation adherence
- Severity of fracture
- Accuracy of fixation
Swelling may persist for several months even after bone healing.
Trimalleolar Fracture Recovery Timeline: Month by Month
Patients and caregivers often want to know what to expect at each stage of recovery. Here is a general guide:
Week 1–2: Focus is on pain control, limb elevation, and swelling reduction. The ankle is immobilised in a splint or cast. No weight bearing is allowed.
Week 2–6: Continued non-weight bearing. Sutures are removed around week 2. X-rays may be taken to confirm fracture position. Gentle toe and knee exercises are started.
Week 6–10: Partial weight bearing begins under physiotherapy guidance, usually with a walking boot and crutches. Range of motion exercises for the ankle start in this phase.
Week 10–12: Most patients progress to full weight bearing with a boot, then transition to normal footwear. Physiotherapy sessions become more active.
Month 3–4: Active strengthening of the ankle, calf, and leg muscles. Balance and proprioception training begins. Many patients return to desk-based work around this time.
Month 4–6: Walking independently is well established. Patients with physical jobs or active lifestyles continue rehabilitation.
Month 6 and beyond: Return to sports and high-demand activities. Some patients continue to notice swelling or mild stiffness beyond 6 months, which is normal.
One year after trimalleolar fracture: Most patients report significant functional improvement. Residual stiffness and occasional swelling can still occur, particularly in complex cases or those with associated dislocation.
Weight Bearing After Trimalleolar Fracture
A very common question from patients is: “When can I put weight on my foot?”
Weight-bearing timelines after trimalleolar fracture surgery generally follow this pattern:
- 0 to 6 weeks: Non-weight bearing – no pressure on the operated ankle
- 6 to 10 weeks: Partial weight bearing – walking with crutches and a boot, gradually increasing load
- 10 to 12 weeks: Full weight bearing in a boot, transitioning to normal shoes
- 12 weeks onward: Walking without aids in most cases
These timelines vary depending on fracture complexity, quality of fixation, bone healing observed on follow-up X-rays, and the surgeon’s assessment. Weight bearing too early can disturb the fixation and delay healing. Always follow the treating surgeon’s specific instructions.
Rehabilitation & Physiotherapy
Rehabilitation is essential for restoring function.
Key components:
- Range of motion exercises
- Strength training
- Proprioception training
- Balance exercises
- Gait correction
- Return-to-sport training
Delayed rehabilitation may result in stiffness and weakness.
Trimalleolar Fracture Recovery Exercises
The following exercises are typically introduced in a phased rehabilitation programme. These should always be done under physiotherapy supervision and not started without medical clearance.
Phase 1 – Early exercises (weeks 2–6, non-weight bearing):
- Toe flexion and extension
- Knee bending and straightening
- Thigh muscle (quad) contractions
- Hip exercises to maintain strength
Phase 2 – Mobility exercises (weeks 6–10):
- Gentle ankle circles and pumps
- Seated towel stretches for the calf
- Active assisted range of motion with the physiotherapist
Phase 3 – Strengthening (weeks 10–16):
- Calf raises (starting with both legs, progressing to single leg)
- Resistance band ankle exercises
- Seated and standing balance exercises
- Step-up and step-down training
Phase 4 – Functional training (month 4–6):
- Single-leg balance on an unstable surface
- Controlled walking on inclines
- Return-to-sport drills for athletes
Consistent physiotherapy following a trimalleolar fracture is one of the most important factors in long-term outcome. Patients who complete structured rehabilitation typically regain better function with fewer long-term complications.
Complications of Trimalleolar Fracture
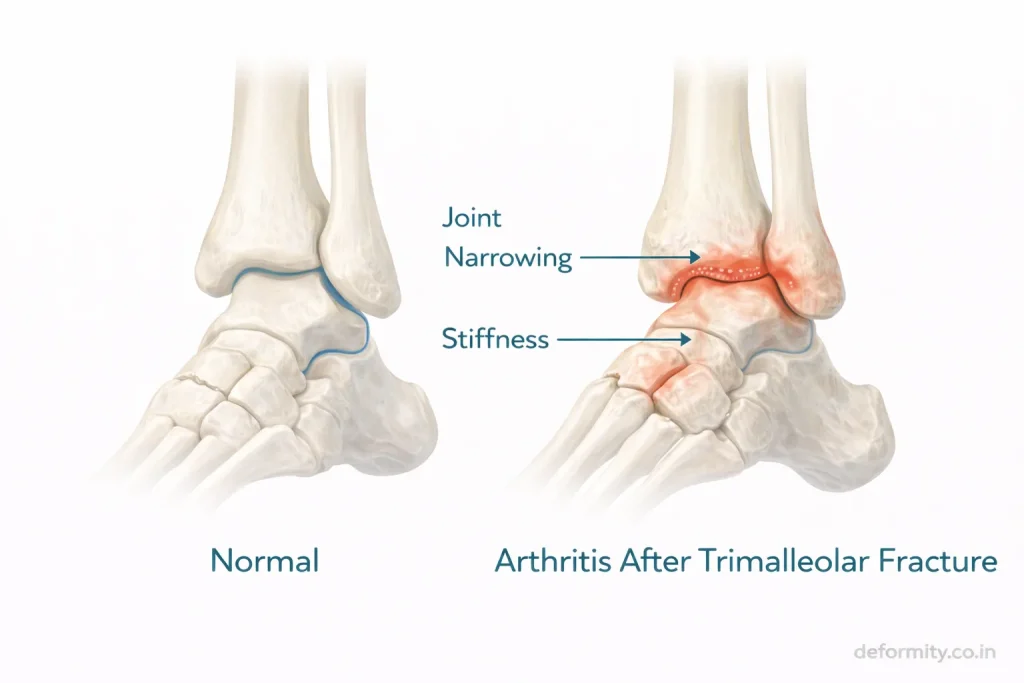
Because this injury involves joint surface disruption, complications may occur.
Possible complications:
- Post-traumatic arthritis
- Malunion
- Nonunion
- Infection
- Hardware irritation
- Chronic pain
- Reduced ankle mobility
Early surgery and structured rehabilitation significantly reduce these risks.
Chronic Pain After Trimalleolar Fracture
Chronic pain is one of the most frequently reported long-term concerns after a trimalleolar fracture. It can arise from several sources:
- Post-traumatic arthritis – cartilage damage at the time of injury accelerates joint wear
- Malunion – if bones heal in a slightly incorrect position, uneven load distribution causes ongoing pain
- Hardware irritation – screws or plates close to tendons can cause aching or tightness
- Nerve involvement – injury to small nerves around the ankle can cause burning, tingling, or persistent discomfort
Chronic pain after trimalleolar fracture should not be dismissed as “normal.” A specialist review including imaging can identify the source and guide appropriate management – whether physiotherapy, medication, or revision intervention.
Nerve Damage After Trimalleolar Fracture
Nerve injury is a less discussed but important complication. The nerves most commonly affected include:
- Superficial peroneal nerve – runs along the outer ankle; injury can cause numbness or tingling on the top of the foot
- Sural nerve – behind the outer ankle; damage causes numbness along the outer edge of the foot
- Tibial nerve – a deeper nerve that may be affected in severe dislocations
Nerve damage after a trimalleolar fracture may present as:
- Numbness or reduced sensation in the foot
- Burning or electric-shock sensations
- Weakness in foot movement
- Hypersensitivity to touch
Most nerve symptoms improve gradually over weeks to months as swelling reduces. Persistent nerve symptoms beyond 3 months should be formally evaluated by a specialist.
Trimalleolar Fracture Prognosis and Long-Term Outcomes
Patients often ask: “Will I ever fully recover?” or “What is my long-term prognosis?”
The honest answer is – most patients do well with appropriate treatment, but outcomes vary based on several factors.
Factors associated with better prognosis:
- Accurate surgical reduction of all three fragments
- Posterior malleolus involving less than 25% of the joint surface
- No associated ankle dislocation
- Younger age and good bone quality
- Consistent rehabilitation
Factors associated with more challenging recovery:
- Large posterior malleolus fragment (>25–30% of joint surface)
- Associated ankle dislocation at the time of injury
- Delayed treatment
- Open fracture or infection
- Pre-existing arthritis or osteoporosis
Long-term outcomes to be aware of:
- Post-traumatic arthritis affects a significant proportion of patients with trimalleolar fractures, even with good surgical reduction
- Most patients regain good walking ability and return to daily activities
- High-demand sport may take 9–12 months to resume
- Some patients experience mild residual stiffness or swelling for 1 to 2 years
The goal of surgery is to give the joint the best possible chance of long-term function. Early, accurate fixation significantly improves the long-term prognosis compared to non-surgical management.
Trimalleolar Fracture Recovery Stories: What Patients Experience
While every recovery is individual, patients commonly describe the following experience:
Months 1–2: The hardest phase – non-weight bearing is frustrating, swelling is significant, and daily tasks require help from family or carers.
Month 3: A turning point for most – weight bearing begins, and there is a visible sense of progress. Physiotherapy starts feeling productive.
Months 4–6: Independence returns gradually. Most patients are walking with normal footwear and managing daily activities without crutches.
Month 6–12: Continued improvement. Patients often describe residual stiffness in the morning, swelling after a long day, and some limitations in walking on uneven ground.
One year and beyond: Most patients have returned to their regular lives. High-demand physical work or sports may take the full 12 months or slightly longer.
The mental aspect of recovery is just as important as the physical. Staying consistent with physiotherapy, managing expectations, and communicating with your surgeon at each follow-up makes a significant difference in the overall experience.
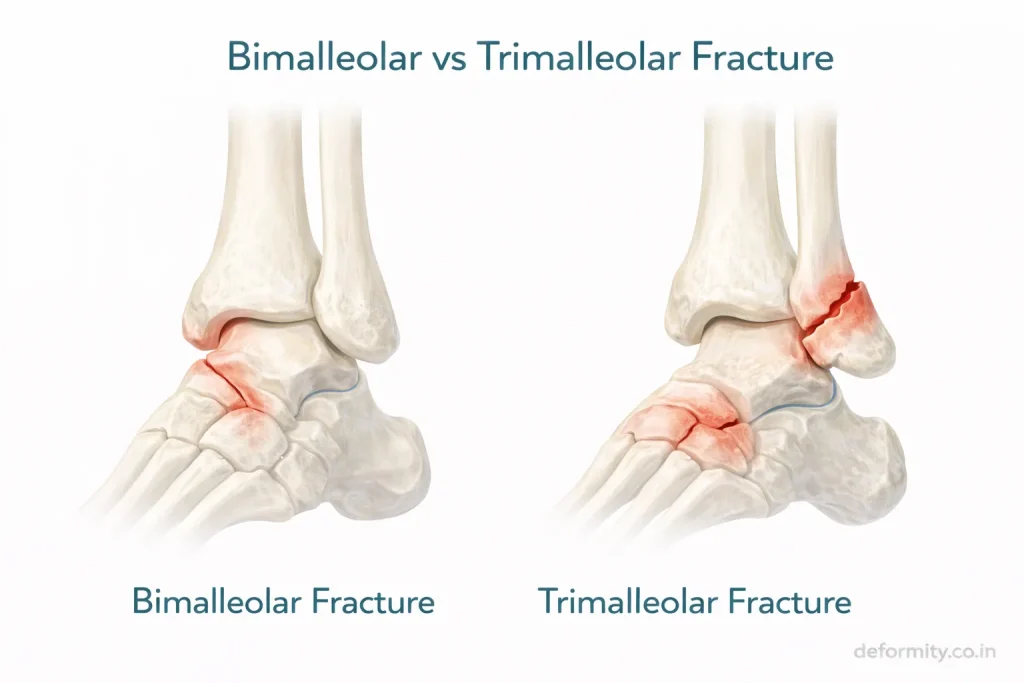
Trimalleolar vs Bimalleolar Fracture
| Feature | Bimalleolar | Trimalleolar |
|---|---|---|
| Bones involved | 2 | 3 |
| Posterior involvement | No | Yes |
| Stability | Unstable | Highly unstable |
| Surgical complexity | Moderate | High |
| Recovery time | 3–6 months | 6–12 months |
Trimalleolar fractures carry a higher risk of arthritis due to posterior joint involvement.
Key Differences: Bimalleolar vs Trimalleolar Fracture
The difference between bimalleolar and trimalleolar fractures is often a source of confusion for patients.
In a bimalleolar fracture, the medial and lateral malleoli are fractured. The posterior malleolus remains intact, which means the back of the ankle joint is still supported. Surgery is still usually required, but the reconstruction is simpler.
In a trimalleolar fracture, all three malleoli are fractured. The posterior joint surface is disrupted, the ankle is highly unstable, and the risk of talar shift is much greater. Surgical complexity is higher, recovery is longer, and the risk of post-traumatic arthritis is greater.
Understanding this difference helps patients know why their treatment and recovery timeline is more involved compared to simpler ankle fractures.
Read more about: Bimalleolar Ankle Fracture: Symptoms, Surgery, Fixation & Recovery
When to Seek Emergency Care
Seek urgent medical attention if:
- Severe ankle deformity
- Intense swelling
- Numbness in toes
- Inability to move the foot
- Severe pain after the accident
Prompt evaluation prevents complications.
Treatment in India & International Consultation
Advanced surgical management is essential for optimal outcomes.
Dr. Divya Ahuja provides specialized treatment for complex ankle injuries, including trimalleolar fractures, witha focus on:
- Anatomical reduction
- Advanced fixation techniques
- Syndesmotic stabilization
- Structured rehabilitation
International patients benefit from:
- Online consultation
- Treatment planning
- Affordable surgery
- Comprehensive post-operative care
Conclusion
A trimalleolar fracture is a complex and unstable ankle injury requiring careful radiological evaluation, surgical fixation, and structured rehabilitation. With timely expert management and consistent physiotherapy, most patients regain functional mobility and return to daily activities. Early treatment is critical to preserve joint health and prevent long-term complications.
Explore all our fracture-related blogs
| Topic | Link |
| Cervical Radiculopathy | Click here |
| Distal Radius Fracture | Click here |
| Proximal Humerus Fracture | Click here |
| Lauge-Hansen Classification of Ankle Fractures | Click here |
| Weber Classification of Ankle Fractures | Click here |
| Trimalleolar Fracture | Click here |
| Bimalleolar Ankle Fracture | Click here |
| Lateral Malleolus Fracture | Click here |
| Medial Malleolus Fracture | Click here |
| Complete Guide to Ankle Fractures | Click here |
| Femur Shaft Fractures | Click here |
| Tibia Fracture | Click here |
FAQs
What is a trimalleolar fracture?
A trimalleolar fracture is a severe ankle injury involving the medial, lateral, and posterior malleoli. It disrupts joint stability and usually requires surgical fixation to restore alignment and prevent long-term complications.
Is a trimalleolar fracture serious?
Yes. Because three parts of the ankle joint are fractured, the injury is highly unstable and requires urgent orthopedic care to prevent chronic pain and arthritis.
Does it always need surgery?
Most trimalleolar fractures require surgery due to instability and joint surface involvement. Rare non-displaced cases may be managed conservatively under close supervision.
How long does trimalleolar fracture recovery take?
Basic healing occurs in 8–12 weeks, but full recovery, including strength and mobility, may take 6–12 months depending on rehabilitation and fracture severity.
What are the radiology findings in a trimalleolar fracture?
Radiology shows fractures of the medial and lateral malleoli along with a posterior tibial fragment. A CT scan helps assess fragment size and joint congruity for surgical planning.
How long does trimalleolar fracture surgery take?
Surgery typically takes 2 to 4 hours depending on fracture complexity, posterior malleolus fixation method, and whether syndesmotic repair is needed.
When can I bear weight after a trimalleolar fracture?
Most patients remain non-weight bearing for 6 weeks, begin partial weight bearing around weeks 6 to 10, and progress to full weight bearing by weeks 10 to 12.
What is the difference between a bimalleolar and a trimalleolar fracture?
A bimalleolar fracture involves two malleoli. A trimalleolar fracture involves all three, including the posterior malleolus, making it more unstable with a longer recovery and higher arthritis risk.
Can a trimalleolar fracture cause chronic pain?
Yes. Chronic pain can result from post-traumatic arthritis, malunion, hardware irritation, or nerve involvement. Persistent pain beyond 3 months should be formally evaluated by a specialist.
What does a trimalleolar fracture feel like?
It causes intense immediate pain, rapid swelling, bruising, visible deformity, and complete inability to bear weight. It is considered one of the most painful ankle injuries.
What is a nondisplaced trimalleolar fracture?
A nondisplaced fracture means the bones cracked but stayed in the correct position. These are rare in trimalleolar injuries but may occasionally be managed without surgery under specialist supervision.
Is a trimalleolar fracture the same as a triple ankle fracture?
Yes. Triple ankle fracture, triple malleolar fracture, and broken ankle in three places are all common ways patients describe the same injury – a trimalleolar fracture.
What causes nerve damage after a trimalleolar fracture?
Nerve damage can result from direct injury at the time of fracture, swelling compressing nearby nerves, or surgical proximity to small nerves. Most symptoms improve over months with monitoring.
What happens one year after a trimalleolar fracture?
Most patients have returned to daily activities by one year. Some residual morning stiffness or swelling after prolonged activity may remain, particularly in complex cases with prior dislocation.
How is a trimalleolar fracture classified?
Trimalleolar fractures are classified using the Weber system (based on fibula fracture level) and the Lauge-Hansen system (based on injury mechanism). Supination-external rotation is the most common pattern.
What is an open trimalleolar fracture?
An open fracture means the bone has broken through the skin. It is a surgical emergency requiring urgent wound debridement and fracture stabilisation to prevent serious infection.
What is external fixation in a trimalleolar fracture?
External fixation is a temporary stabilisation method using pins and rods outside the skin. It is used when swelling, open wounds, or the patient’s condition prevent immediate definitive surgery.
What is the prognosis for a trimalleolar fracture?
Most patients regain good function with accurate surgery and rehabilitation. Risk of post-traumatic arthritis remains, particularly with large posterior fragments or associated ankle dislocation.