The Lauge-Hansen classification is a mechanism-based system used to describe ankle fractures. Unlike the Weber classification, which focuses on the level of fibular fracture, the Lauge-Hansen ankle fracture classification explains how the injury occurred, based on foot position and direction of deforming force.
This system is widely taught in orthopedic training, radiology, and trauma education because it helps predict fracture patterns, ligament injuries, instability, and surgical requirements. One of the most commonly searched patterns is the SE4 ankle fracture (Supination–External Rotation Stage IV), which represents a completely unstable injury.
In this comprehensive guide, you’ll learn:
Table of Contents
What is the Lauge-Hansen Classification?
The Lauge-Hansen classification was developed by Danish orthopedic surgeon Niels Lauge-Hansen. It categorizes ankle fractures based on the mechanism of injury, not just fracture location.
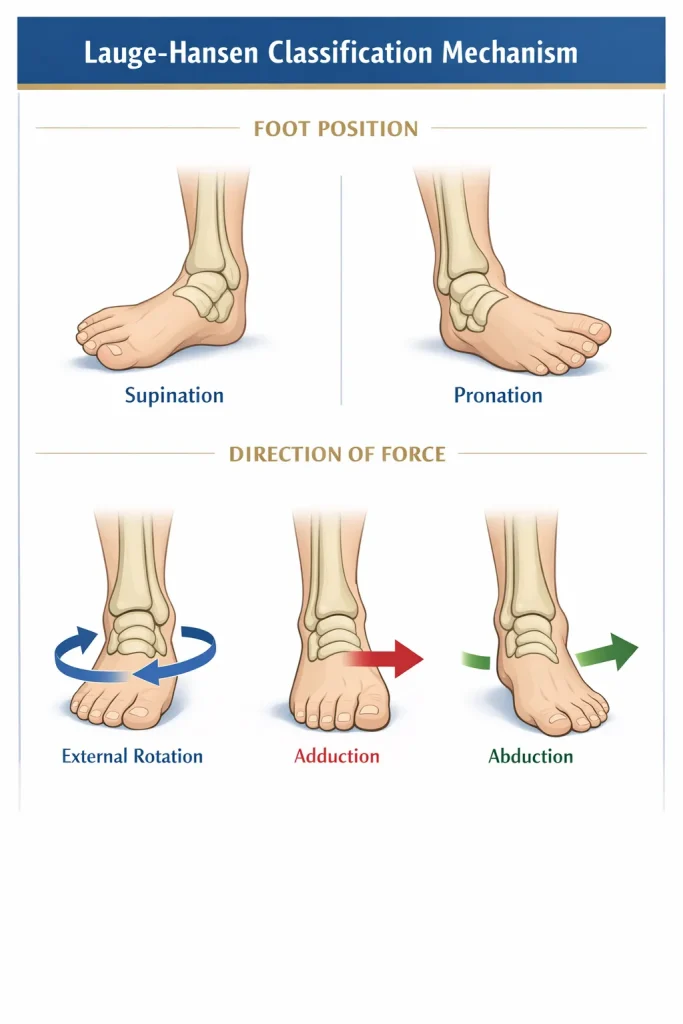
Each injury pattern is named using two components:
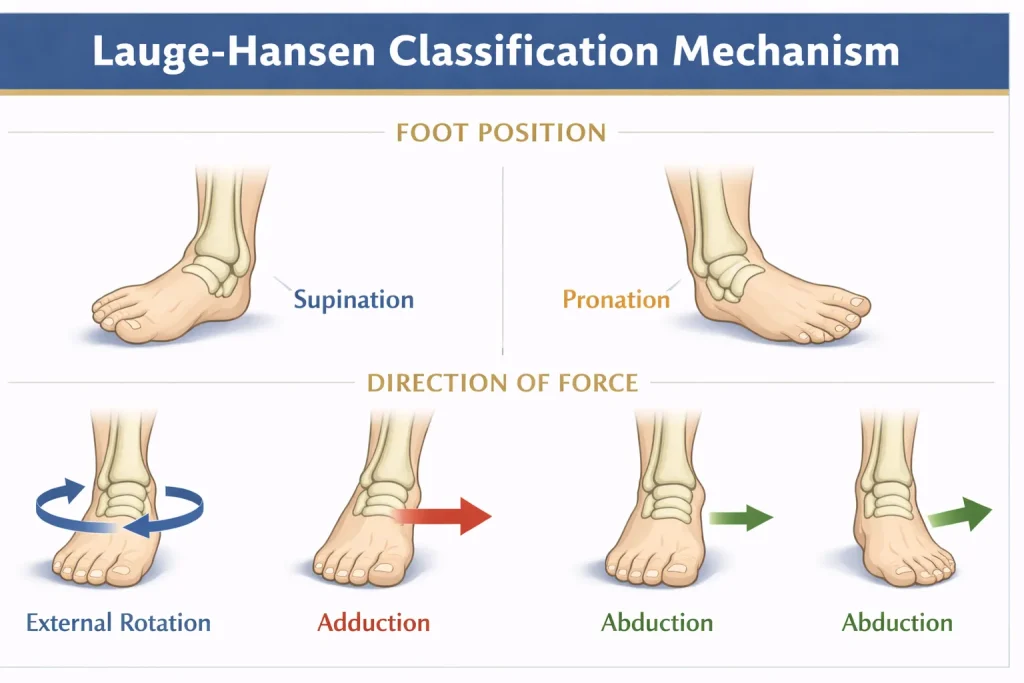
- Foot position at time of injury
- Supination
- Pronation
- Direction of applied force
- External rotation
- Adduction
- Abduction
For example:
Supination–External Rotation (SER)
This means the foot was supinated, and an external rotational force caused the injury.
Basic Principles of the Lauge-Hansen System
The classification follows a logical sequence:
- First word = foot position
- Second word = direction of force
- Injury progresses in stages
Each mechanism progresses through predictable stages of structural failure.
Typical stage progression:
- Stage I → ligament injury or minor fracture
- Stage II → fibular fracture
- Stage III → posterior malleolus injury
- Stage IV → medial malleolus fracture or deltoid ligament rupture
This sequential progression helps predict associated injuries and instability.
Types of Lauge-Hansen Ankle Fractures
There are four primary patterns in the Lauge-Hansen classification:
- Supination–External Rotation (SER)
- Supination–Adduction (SA)
- Pronation–External Rotation (PER)
- Pronation–Abduction (PA)
Supination–External Rotation (SER)

This is the most common ankle fracture mechanism.
Mechanism
- Foot in supination
- External rotational force applied
Stage Progression
Stage I – Anterior inferior tibiofibular ligament injury
Stage II – Oblique fibular fracture (Weber B type)
Stage III – Posterior malleolus fracture
Stage IV – Medial malleolus fracture or deltoid ligament rupture
An SER4 ankle fracture represents complete instability.
Supination–Adduction (SA)

Mechanism
- Supinated foot
- Adduction force
Injury Pattern
- Transverse fibular fracture below the syndesmosis
- Vertical medial malleolus fracture
This pattern may be unstable depending on displacement.
Supination – Adduction Ankle Fracture Pattern: What Makes It Unique
The supination-adduction (SA) pattern is less common than SER but clinically important because it produces a vertical shear fracture of the medial malleolus – a feature not seen in other Lauge-Hansen patterns.
Key distinguishing points:
- The fibular fracture in SA is transverse and below the level of the joint (infra-syndesmotic), often a Weber A equivalent
- The medial malleolus fracture runs vertically, caused by axial loading and adduction force
- The syndesmosis is typically intact, making this injury more stable than PER or SER4
- However, the vertical medial malleolus fragment can be difficult to fix and may require lag screw fixation
On X-ray, look for a low transverse fibular fracture combined with a steep, vertical medial malleolus fracture line. This combination is essentially diagnostic of the SA pattern.
Surgically, the vertical medial malleolus fracture in SA often requires buttress plating rather than simple lag screws, because axial load can cause fracture collapse if only screws are used.
Pronation–External Rotation (PER)

Mechanism
- Foot pronated
- External rotational force
Injury Pattern
- Medial malleolus fracture or deltoid ligament injury
- High fibular fracture (similar to Weber C)
- Syndesmotic disruption
PER injuries are often unstable and surgical.
PER Lauge-Hansen: Fibular Fracture Level and Syndesmotic Injury
A commonly asked question in radiology and orthopedic exams is: “In the Lauge-Hansen classification system, what is the typical fibular fracture pattern seen with a pronation–external rotation injury to the ankle?”
The answer: In PER injuries, the fibular fracture is high – above the level of the syndesmosis, at or proximal to the proximal fibula in advanced cases (Maisonneuve fracture pattern). The fracture is typically spiral or oblique, and the key distinguishing feature is that the injury begins medially, with the deltoid ligament or medial malleolus failing first.
The injury sequence in PER is:
- Stage I – Medial malleolus fracture or deltoid ligament rupture
- Stage II – Anterior inferior tibiofibular ligament disruption (and interosseous membrane)
- Stage III – Posterior inferior tibiofibular ligament tear or posterior malleolus fracture
- Stage IV – High fibular fracture (spiral, above syndesmosis)
Because the fibular fracture in PER can be very high – even at the fibular neck – it is easy to miss on standard ankle X-rays. Always request a full-length fibula X-ray when medial-sided ankle injury is present without a visible fibular fracture on standard views. Missing the fibular fracture means missing a Maisonneuve-equivalent injury, which is highly unstable.
Pronation–Abduction (PA)

Mechanism
- Foot pronated
- Abduction force
Injury Pattern
- Transverse medial malleolus fracture
- Comminuted fibular fracture
- Syndesmotic injury
These fractures are typically unstable.
SE4 Ankle Fracture Explained

The term SE4 ankle fracture refers to:
Supination–External Rotation Stage IV
This represents a complete injury pattern involving:
- Fibular fracture (Weber B type)
- Posterior malleolus fracture
- Medial malleolus fracture or deltoid ligament rupture
SE4 injuries are:
- Highly unstable
- Frequently require surgery
- Common in twisting injuries
Radiologically, SE4 shows:
- Oblique fibular fracture
- Posterior fragment
- Medial clear space widening
Because of instability, surgical fixation is commonly required.
SER IV vs SE4: Are They the Same?
Yes – SER IV, SE4, SER4, and Ser Type 4 all refer to the same injury: Supination–External Rotation Stage IV. These terms are used interchangeably in clinical practice and orthopedic literature.
The abbreviation varies by region and institution:
- “SER IV” or “SER4” is the most technically accurate short form
- “SE4” is commonly used in radiology reports and exam questions
- “Ser Type 4” appears in some textbooks
All of these describe the same complete, unstable bimalleolar or trimalleolar equivalent ankle fracture pattern. If you encounter any of these terms on an X-ray report or exam question, they are describing the same injury – and the clinical implication is the same: likely surgical management required.
Lauge-Hansen Mnemonic

Remembering all patterns can be challenging, so mnemonics help.
Simple Pattern Mnemonic:
“Some Say Please Pass”
- S – Supination External Rotation (SER)
- S – Supination Adduction (SA)
- P – Pronation External Rotation (PER)
- P – Pronation Abduction (PA)
Another learning trick:
Foot position always comes first.
Force direction comes second.
Stage-Specific Mnemonic for SER (Most Common Pattern)
To remember the four stages of Supination-External Rotation:
“All Fractures Produce Mayhem”
- A – Anterior inferior tibiofibular ligament (Stage I)
- F – Fibular fracture, oblique (Stage II)
- P – Posterior malleolus fracture (Stage III)
- M – Medial malleolus fracture or deltoid rupture (Stage IV)
This mnemonic helps students and residents recall the sequential progression of SER injuries, which is the most tested pattern in orthopedic and radiology exams.
Lauge-Hansen vs Weber Classification

Both systems classify ankle fractures, but differently.
| Feature | Lauge-Hansen | Weber |
|---|---|---|
| Basis | Mechanism | Fracture level |
| Focus | Foot position + force | Syndesmosis level |
| Complexity | Higher | Simpler |
| Clinical use | Predicts progression | Guides stability |
Example correlation:
- SER fractures often correspond to Weber B fractures
- PER fractures often correspond to Weber C fractures
Using both systems together improves understanding.
Weber-Lauge-Hansen Correlation: A Practical Guide
Many clinicians use both systems simultaneously because they complement each other. Here is a practical correlation guide:
| Lauge-Hansen Pattern | Typical Weber Equivalent | Syndesmosis Status |
|---|---|---|
| SA (Supination–Adduction) | Weber A | Intact |
| SER I–II (Supination–External Rotation) | Weber B | Usually intact |
| SER III–IV (Supination–External Rotation) | Weber B | At risk or disrupted |
| PA (Pronation–Abduction) | Weber B or C | Disrupted |
| PER (Pronation–External Rotation) | Weber C | Disrupted |
The key insight: Weber tells you where the fracture is. Lauge-Hansen tells you why it is there and what else might be injured.
Weber B fractures, for example, can result from either SER or PA mechanisms – and the treatment implications are different. A Weber B from SER II may be managed conservatively, while a Weber B from SER IV requires surgery. This is why Lauge-Hansen adds clinical value beyond Weber alone.
Read more about: Weber Classification of Ankle Fractures: Types A, B & C Explained
Lauge-Hansen Classification Radiology Guide
Radiology is essential for identifying fracture patterns.
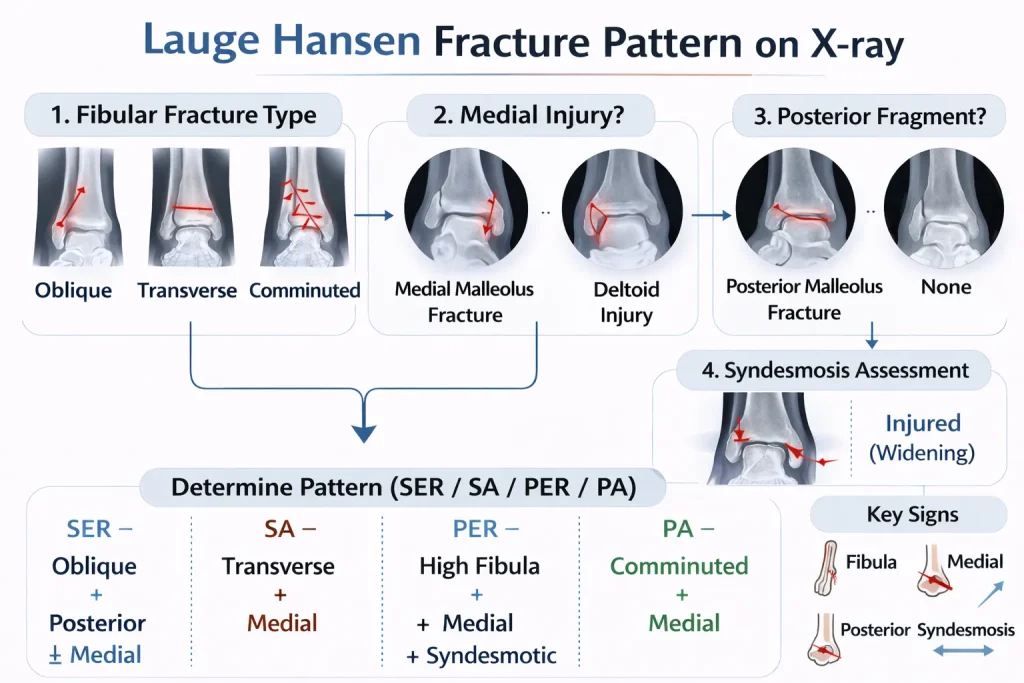
How to Identify the Lauge-Hansen Pattern on X-ray
Steps:
- Identify fibular fracture type
- Check the medial malleolus
- Assess posterior malleolus
- Evaluate syndesmosis
Pattern recognition is key.
Radiographic Progression by Stage

Stage I – ligament injury (may not be visible)
Stage II – fibular fracture
Stage III – posterior malleolus involvement
Stage IV – medial fracture or deltoid rupture
A CT scan may be required to assess posterior fragments.
Lauge-Hansen Classification Radiology: Pattern Recognition on X-ray and CT
Understanding what to look for on imaging is essential for correct classification. Here is a systematic radiology approach for each pattern:
SER (Supination–External Rotation) – Radiographic Features:
- Fibular fracture is oblique or spiral, at the level of the syndesmosis (Weber B equivalent)
- The fracture line runs from anteroinferior to posterosuperior on lateral view
- Medial clear space may be widened in Stage IV (deltoid rupture)
- Posterior malleolus fragment visible on lateral X-ray in Stage III–IV
- Stress views or MRI may be needed to detect Stage I (ligament injury – invisible on plain X-ray)
PER (Pronation–External Rotation) – Radiographic Features:
- Medial-sided injury first: transverse medial malleolus fracture or widened medial clear space
- Fibular fracture is high – above the joint line, often proximal to the syndesmosis
- In Maisonneuve pattern, the fibular fracture may be at the fibular neck – only visible on full-length views
- Syndesmotic widening: tibiofibular clear space >6mm, tibiofibular overlap <10mm on AP view
SA (Supination–Adduction) – Radiographic Features:
- Transverse fibular fracture below the joint line (infra-syndesmotic, Weber A equivalent)
- Vertical fracture line through the medial malleolus
- No syndesmotic widening
PA (Pronation–Abduction) – Radiographic Features:
- Transverse medial malleolus fracture
- Comminuted or transverse fibular fracture at or above the syndesmosis
- Potential syndesmotic widening
CT Scan Indications: CT is indicated when:
- Posterior malleolus fragment size needs precise assessment (>25% articular involvement = surgical)
- Syndesmotic injury is suspected but not confirmed on X-ray
- Comminution is present and surgical planning is needed
- Fracture pattern does not fit cleanly into one category
MRI Role in Lauge-Hansen Assessment: MRI is useful for Stage I injuries where only ligament damage has occurred and X-rays appear normal. It can confirm anterior inferior tibiofibular ligament tears, deltoid ligament ruptures, and occult fractures that plain X-ray misses.
Posterior Malleolus Fracture in Lauge-Hansen Classification
The posterior malleolus is involved in Stage III of the SER pattern and also in PER injuries. Its classification and management are important enough to address separately.
Why Does the Posterior Malleolus Fracture?
In SER injuries, the posterior inferior tibiofibular ligament (PITFL) either avulses the posterior malleolus or transmits force directly to it as the talus rotates externally. The fragment size varies from a small avulsion to a large fragment involving >25–30% of the articular surface.
Posterior Malleolus Classification Within Lauge-Hansen
- Small avulsion fragment (<25% articular surface): Often managed non-operatively if the ankle is otherwise stable after fibular fixation
- Large fragment (>25% articular surface): Requires fixation to restore joint congruity and prevent talar subluxation
- Volkmann fragment (posterior plafond fracture): Extends further and involves the posterior articular surface — requires CT and careful surgical planning
The posterior malleolus is sometimes called the “third malleolus” and its involvement converts a bimalleolar fracture into a trimalleolar fracture pattern.
Surgical Fixation of the Posterior Malleolus
Two main approaches exist:
- Anterior-to-posterior lag screws: Commonly used for smaller fragments accessible with fluoroscopy
- Posterolateral plating: Preferred for larger, comminuted, or articular fragments requiring direct visualization
CT scan is mandatory before deciding on posterior malleolus fixation strategy.
Pott’s Fracture and the Lauge-Hansen Classification
A question that appears in orthopedic exams and clinical discussions is: “Where does Pott’s fracture fit in the Lauge-Hansen classification?”
Pott’s fracture is a historical term describing a bimalleolar ankle fracture – typically involving both the fibula and the medial malleolus. It was described by Percivall Pott in 1765, long before Lauge-Hansen’s work.
In modern classification terms, Pott’s fracture most closely corresponds to SER Stage IV (SE4) – involving a fibular fracture and medial malleolus fracture (or deltoid ligament injury).
However, the term Pott’s fracture is non-specific and can also overlap with:
- PA (Pronation–Abduction) patterns if abduction was the mechanism
- PER patterns in high-energy injuries with syndesmotic disruption
The Lauge-Hansen classification effectively replaced the descriptive use of “Pott’s fracture” in modern orthopedics by providing a mechanistic framework that predicts associated ligament injuries and guides treatment.
Today, “Pott’s fracture” is used loosely in some clinical settings but is not an accepted classification term. When encountered, it should be correlated with the Lauge-Hansen pattern based on mechanism and imaging.
Clinical Relevance of Lauge-Hansen Classification
The classification is clinically valuable because it:
- Predicts instability
- Anticipates ligament injury
- Guides surgical planning
- Helps explain the mechanism to patients
Understanding the mechanism helps surgeons anticipate associated injuries.
Dr Divya Ahuja uses mechanism-based assessment along with radiology to plan optimal fixation in complex ankle fractures.
Treatment Based on Lauge-Hansen Pattern
Treatment depends on stage and stability.
- SER I–II → may be stable
- SER III–IV → unstable, often surgical
- PER injuries → usually surgical
- PA injuries → commonly surgical
Surgical treatment may include:
- ORIF (Open Reduction and Internal Fixation)
- Plate fixation
- Syndesmotic screw
- Posterior malleolus fixation
Recovery & Prognosis
Recovery depends on:
- Fracture severity
- Number of stages involved
- Ligament injury
- Surgical accuracy
- Rehabilitation adherence
Typical timeline:
- 6 weeks non-weight bearing
- 8–12 weeks of gradual walking
- 3–6 months rehabilitation
- 6–12 months full recovery
SE4 injuries may require longer recovery.
Complications
Possible complications include:
- Post-traumatic arthritis
- Chronic instability
- Syndesmotic failure
- Malunion
- Nonunion
Early treatment reduces long-term risks.
Treatment in India & International Consultation
Complex ankle fractures require careful evaluation and anatomical fixation.
Dr Divya Ahuja specializes in:
- Mechanism-based fracture assessment
- Complex ankle trauma fixation
- Syndesmotic stabilization
- Advanced rehabilitation planning
International patients benefit from:
- Online consultations
- Surgical planning
- Affordable treatment options
- Comprehensive postoperative care
Conclusion
The Lauge-Hansen ankle fracture classification provides deep insight into the mechanism of injury and predictable fracture progression. By understanding foot position, force direction, and stage progression, clinicians can better predict instability, plan treatment, and improve outcomes. When combined with radiological evaluation and modern surgical techniques, it remains a powerful tool in ankle trauma management.
Explore all our fracture-related blogs
| Topic | Link |
| Cervical Radiculopathy | Click here |
| Distal Radius Fracture | Click here |
| Proximal Humerus Fracture | Click here |
| Lauge-Hansen Classification of Ankle Fractures | Click here |
| Weber Classification of Ankle Fractures | Click here |
| Trimalleolar Fracture | Click here |
| Bimalleolar Ankle Fracture | Click here |
| Lateral Malleolus Fracture | Click here |
| Medial Malleolus Fracture | Click here |
| Complete Guide to Ankle Fractures | Click here |
| Femur Shaft Fractures | Click here |
| Tibia Fracture | Click here |
FAQs
What is Lauge-Hansen’s classification of ankle fractures?
Lauge Hansen classification is a mechanism-based system that categorizes ankle fractures according to foot position and direction of force at the time of injury. It includes patterns like Supination-External Rotation and Pronation-External Rotation.
What does SE4 ankle fracture mean?
SE4 stands for Supination–External Rotation Stage IV, representing a completely unstable ankle fracture involving fibular fracture, posterior malleolus injury, and medial malleolus fracture or deltoid ligament rupture.
What is the Lauge Hansen mnemonic for easy recall?
A common mnemonic is “Some Say Please Pass,” representing Supination-External Rotation (SER), Supination-Adduction (SA), Pronation-External Rotation (PER), and Pronation-Abduction (PA) fracture patterns.
How is Lauge Hansen’s classification different from Weber’s classification?
Lauge Hansen classification is based on injury mechanism, while Weber classification is based on the level of fibular fracture relative to the syndesmosis. Both systems complement each other in ankle fracture assessment.
Which Lauge Hansen fracture pattern is most common?
Supination–External Rotation (SER) is the most common Lauge-Hansen ankle fracture pattern, often corresponding to Weber B fractures and progressing through four predictable stages.
Is the SE4 ankle fracture considered unstable?
Yes, SE4 ankle fractures are typically unstable because they involve multiple structural failures, including medial and posterior components, and often require surgical fixation.
How many stages are there in the Lauge-Hansen classification?
Most Lauge Hansen patterns progress through four stages, starting with ligament injury and progressing to fibular fracture, posterior malleolus involvement, and medial malleolus fracture.
How do you identify the Lauge Hansen pattern on X-ray?
Identification involves analyzing fibular fracture type, medial malleolus involvement, posterior fragment presence, and syndesmotic widening on ankle X-rays.
What is a supination external rotation ankle fracture?
Supination External Rotation fracture occurs when the foot is supinated and external rotational force is applied, leading to predictable staged injury progression, commonly ending in SER4 pattern.
Is Lauge Hansen classification still used in modern orthopedics?
Yes, Lauge Hansen classification remains relevant in orthopedic training and trauma assessment because it explains fracture mechanism and predicts associated ligament injuries.
What is the fibular fracture pattern in pronation–external rotation (PER) injuries?
In PER injuries, the fibular fracture is high – above the syndesmosis – and is typically spiral or oblique. In advanced cases it can occur at the fibular neck (Maisonneuve pattern). The injury begins medially, making it critical not to miss a high fibular fracture when medial ankle injury is present.
What is Pott’s fracture in relation to Lauge-Hansen classification?
Pott’s fracture is a historical term for bimalleolar ankle fracture. In modern terms, it most closely corresponds to SER Stage IV (SE4) in the Lauge-Hansen classification. The term is non-specific and has largely been replaced by mechanism-based Lauge-Hansen terminology in contemporary orthopedics.
Are SER4, SE4, SER IV, and Ser Type 4 the same injury?
Yes. SER4, SE4, SER IV, and Ser Type 4 are all abbreviations for the same injury – Supination–External Rotation Stage IV. They are used interchangeably in clinical practice, radiology reports, and orthopedic examinations.